
by Jake Seegers | Jun 24, 2026 | General
The article below is reprinted with permission from the Clallam County Watchdog. It is one in a series of stories about the growing substance abuse problems (and deaths) in Clallam County, which according to Watchdog reporting have risen in tandem with programs promoted by Dr. Allison Berry.
Berry is Health Officer for both Clallam and Jefferson counties. Under her watch — which critics contend has normalized, facilitated and prolonged active drug addiction — scenes like these are increasingly common in Clallam County:
“What began as a syringe exchange evolved into a comprehensive Harm Reduction Health Center that distributes supplies for virtually every method of drug consumption.
Today, participants receive syringes, smoking supplies, foil, naloxone, boofing kits, and other drug-use supplies. “How-to” literature not only explains alternative methods of consumption, but details how to achieve the most effective high…
In 2018, the county’s syringe exchange had no dedicated employees and a modest budget of just over $60,000.
By 2025, the Harm Reduction Health Center employed four full-time staff and operated on a budget of $531,010 per year…
Meanwhile, overdose deaths in Clallam County have more than tripled since 2018.”
This article examines Health Officer Berry’s effort through a grant to add a mobile unit carrying a specialized drug-testing machine which would have expanded the scope of the “harm reduction” program, reaching into Jefferson County.
“[T]he drug-testing machine would eventually be integrated into harm reduction’s planned mobile van. In partnership with Jefferson County, the mobile unit would provide drug testing and distribute supplies throughout both counties.”
This expanded program was stopped by a single conscientious employee who documented legal liabilities. Testing results require skilled interpretation by trained personnel and false negatives could result in death or injury to drug users. The county, by returning the tested drug to the user, would be responsible for those deaths and injuries.
Public records shown in the Watchdog article reveal how Berry nonetheless:
• disregarded both grant requirements and training materials which stressed that a qualified Drug Technician was needed to operate the drug-testing machine;
• actively promoted the program months before final approval was granted;
• argued to move forward with the program even after liability issues were documented, so that grant money did not “sit wasted” and to prevent “demoralizing” staff.
Health Officer Berry continues to defend these programs. Additional Clallam County Watchdog articles on this subject are linked at bottom.
— The Editors
———————————————————-
Public records reveal how Clallam County nearly became a government-run drug testing service — and the employee who stopped it.
by Jake Seegers
Harm Reduction Almost Broke Clallam County
When Health Officer Allison Berry was appointed in 2018, Clallam County’s harm reduction program was relatively simple: participants exchanged used syringes for clean needles on a one-for-one basis.
The stated goal was straightforward: reduce the spread of HIV, hepatitis, and other bloodborne diseases among people who were already injecting drugs.
Over the next eight years, however, Health Officer Berry and the Clallam County commissioners steadily expanded harm reduction far beyond its original scope. What began as a syringe exchange evolved into a comprehensive Harm Reduction Health Center that distributes supplies for virtually every method of drug consumption.
Today, participants receive syringes, smoking supplies, foil, naloxone, boofing kits, and other drug-use supplies. “How-to” literature not only explains alternative methods of consumption, but details how to achieve the most effective high.
The transformation of a simple disease-prevention strategy into a distribution center for drug-use supplies and resources did not happen by accident. It was the result of a deliberate and sustained effort to expand harm reduction at nearly every opportunity.
Health Officer Berry and the commissioners frequently justified each expansion as a necessary response to the worsening overdose crisis. Yet at every stage, the same question received little discussion:
At what point does reducing the harms of drug use become facilitating drug use itself?
For the Health Officer and the sitting commissioners, there appears to be no limit to their commitment to expanding harm reduction.
That commitment reached a new level in 2023 when Clallam County joined the University of Washington’s ADAI (Addiction, Drugs, and Alcohol Institute) Drug Checking Project. Commissioners Randy Johnson, Mark Ozias, and Mike French unanimously approved the grant-funded program that could have exposed county taxpayers to millions of dollars in liability. [Click here for Community Drug Checking Network Project Site Scope of Work original source.]
Take a Ride in My Drug-Testing Machine
In late 2022, Health Officer Berry began advocating for a grant-funded portable drug-testing machine, also known as a mass spectrometer.
During a December commissioner work session, she stated that the purpose was to better inform response efforts. Berry’s statements, along with her emails, indicated that the county prosecutor, Sheriff’s Office, Port Angeles Police Department, and others had signed off on the program.
The problem with these claims was twofold.
First, the Sheriff’s Office, Port Angeles Police Department, and Coroner’s Office would not have access to the machine. The spectrometer was intended exclusively for the Harm Reduction Health Center.
If the primary goal was data collection, why exclude the very agencies that routinely encounter illegal drugs through investigations, arrests, and overdose deaths?
Second, an email from then-County Administrator Rich Sill indicates that the Sheriff had raised concerns that returning drugs to participants after testing could be unlawful under Washington law.
An individual who delivers an illegal substance to someone who later dies from using it may be charged with controlled substances homicide under RCW 69.50.415.
While ESSB 5536 would later take effect in August 2023, providing protections for public-health employees involved in distributing harm-reduction supplies and testing illegal substances, it did not explicitly provide protections for returning drugs to participants after testing.
The drug-checking program was scheduled to begin before those protections took effect. It also would have launched during the worst overdose period in Clallam County’s history. According to the Coroner’s Office, trailing-twelve-month (TTM) overdose deaths peaked between April 2023 and March 2024, with 51 deaths during that period.
That equates to nearly one overdose death every week.
What were the chances that one of those individuals would have used the drug-checking program? If a participant received a contaminant-free result and later died, could county employees face legal exposure under RCW 69.50.415?
The potential legal and financial liability was significant.
Yet liability concerns appeared to carry little weight. In fact, nearly a year before ESSB 5536 took effect, the county had already begun distributing drug-use supplies beyond syringes as part of its ongoing expansion of harm reduction.
The Process
When the drug-checking program was presented to commissioners during a January 30, 2023 work session, Commissioner Johnson asked the obvious question:
“That’s great, but where are they [illegal drugs] coming from, the Sheriff’s office?”
Karissa McLane, then Public Health Nurse Supervisor for Clallam County Health and Human Services (HHS), explained that participants in the county’s harm reduction program would bring their own drugs in for testing.
A month earlier, during a December 12, 2022 work session, then-Commissioner Bill Peach asked:
“If it turns out that it is illegal drugs, can they get arrested?”
McLane responded:
“That’s a good question. Yes. People can bring their drugs in to get tested. We’ve consulted with our prosecuting attorney’s office and discussed with our sheriff’s office and have determined that people will not be arrested for bringing drugs in to get tested from us.”
The proposed process was straightforward:
- An individual acquires illegal drugs — possibly from any of several open-air drug markets in Port Angeles, like Safeway or the Veterans Bell.
- They bring those drugs to the Harm Reduction Health Center.
- A county health employee tests them using the mass spectrometer.
- The results are shared with the participant.
- The drugs are returned to the participant for use.
The problem is that sophisticated testing by a trusted county health professional can create a false sense of safety when contaminants are not detected. Liability disclosures attempted to address this by explaining that a test result “doesn’t always mean a drug is safe to use.”
But common sense would suggest a simpler message:
“Drugs are never safe to use.”
“Fentanyl will kill you. Don’t use it.”
Yet participants were unlikely to hear such unequivocal language. “Harm Reduction Messaging” guidelines attached to emails obtained through a public records request cautioned:
“When discussing harm reduction, it is important to choose your language carefully to ensure that you are not coming across as paternal, shaming or denigrating.”
When a participant hands illegal drugs to a trusted county health professional, receives a contaminant-free result, and leaves with those drugs—along with a pipe, syringe, or boofing kit—the message received is clear:
Go ahead and use it. It’s been checked.
Blinders
But what would have happened if a county health employee deemed a drug contaminant-free and the participant later died from an overdose?
The answer could have been millions of dollars in liability, litigation costs, settlements, and judgments ultimately borne by taxpayers.
The potential exposure extended beyond Clallam County.
During a January 2023 commissioner work session, Karissa McLane explained that the drug-testing machine would eventually be integrated into harm reduction’s planned mobile van. In partnership with Jefferson County, the mobile unit would provide drug testing and distribute supplies throughout both counties.
After the presentation, Commissioner Ozias asked:
“Commissioners, any other questions?”
The audience could have heard a pin drop.
On February 7, 2023, Commissioner Johnson moved to approve the program; Commissioner French seconded, and the board unanimously approved it without further discussion.
Following the vote, Commissioner Ozias enthusiastically remarked:
“[This] is really exciting! It’s really exciting to see the University [of Washington] being engaged so broadly and directly in communities like our county. I really appreciate that. So, thanks to our public health team for facilitating this.”
Just a Matter of Time
Despite the liability risks, Health Officer Berry and HHS appeared to downplay the importance of having a qualified technician operate the drug-testing machine. While discussing the grant, Berry wrote:
“I am less interested in hiring our own tech.”
Lisa Al-Hakim, then-Prevention Specialist/SSP Coordinator for Clallam County Public Health, proposed an alternative. The Hepatitis Education Project (HEP), a Seattle nonprofit and fellow ADAI Drug Checking Grant recipient, had hired an “OD Prevention Coordinator” instead of a dedicated technician.
The decision appears to have been driven by cost and long-term harm reduction sustainability. Al-Hakim wrote:
“So it looks like HEP hired a OD prevention specialist and rolled their drug-checking tech work into that, which isn’t a bad idea thinking along the lines of sustainability for the harm reduction health program.”
Clallam County followed HEP’s lead.
The problem is that the Drug Checking Network grant specifically required a Drug Technician.
And, Clallam County’s scope of work committed to hiring one.
Instead, the OD Prevention Coordinator position emphasized lived experience and social-service work rather than technical qualifications.
But technical expertise was critical to interpreting the spectrometer’s results.
Before a training session led by Yarelix Estrada of the New York City Department of Health, internal emails acknowledged that interpreting the machine’s spectra readings required experience. The training materials warned:
“We do not trust machines. Do not take the first match and assume it to be true. The art of drug-checking is in the technician’s ability to think critically about the sample and OPUS is only a tool.”
Drug checking was not simply a matter of pushing a button. It required the judgment and critical analysis of a trained technician.
Instead of prioritizing technical expertise, the county specifically encouraged individuals with personal histories of substance use to apply.
Additionally, the position description stated that candidates “must be comfortable handling drug samples and potentially being exposed to substances.”
Encouraging individuals in recovery to apply for a position that requires handling the very drugs they were attempting to avoid does not seem like harm reduction.
The drug-testing machine would have become part of the county’s mobile harm reduction van, with complex analyses potentially conducted not by a Drug Technician, as discussed in the grant, but by an outreach coordinator—possibly someone in recovery—who would handle a constant flow of illegal drugs. That employee would have been responsible for interpreting results, giving drugs to participants, and communicating whether or not contaminants had been detected.
It is difficult to imagine a scenario carrying greater potential for error—or greater liability for Clallam County taxpayers.
A Voice in the Desert
While county officials pressed forward with expanding harm reduction despite significant liability concerns, one employee stepped forward to protect the county from itself.
When Tom Reyes, Deputy Director of Human Resources and Risk Management, learned of the drug-checking program, he immediately recognized the risks and voiced his concerns:
“I believe it is only a matter of time before a lawsuit is filed on someone, or some agency, providing testing. I hope Clallam County is not that first!”
Also of concern, most of the other participants in the ADAI drug-checking program were NGO’s, not government departments.
In the same email, Reyes noted:
“An internet search indicates they are a 501(c) (3), not a County entity. Clearly, they would not have the same level of risk exposure.”
A former detective with the Clallam County Sheriff’s Office, Reyes acted quickly despite apparent internal pressure to dismiss the liability concerns. He contacted Derek Bryan of the Washington Counties Risk Pool, the insurer that provides coverage for Clallam County.
Less than a week later, a response from Ken Kollmann effectively stopped the program in its tracks.
The county dodged a bullet—one that its Health Officer and commissioners had been willing to put the county in front of.
Common Sense Prevails
The drug-checking machine was never the real story.
The story is how far county leadership was willing to go in its effort to expand harm reduction.
Public records show that pursuit of the ADAI Drug Checking Grant was part of a broader, coordinated effort to grow harm reduction services in Clallam County.
The Harm Reduction Health Center had already taken possession of the machine and was actively promoting the program months before final approval was granted.
When the program encountered resistance, Health Officer Berry attempted to salvage it by appealing to the pity of Tom Reyes:
“Our staff are already incredibly overstretched and watching this position go unfilled and the money sit wasted has been deeply demoralizing to them. We cannot afford to lose any more staff to burnout this year.”
But Reyes understood what others seemed unwilling to acknowledge. As Deputy Director of Human Resources and Risk Management and a former Sheriff’s Office detective, he recognized the extraordinary liability being created by a county-operated drug-checking program.
While commissioners and public health officials focused on expanding harm reduction, Reyes focused on legality, liability, and common sense.
He elevated his concerns to the Washington Counties Risk Pool, and within days, the program was effectively dead.
Although Clallam County had already acquired the machine, it was ultimately returned to the University of Washington. The county dodged a potentially catastrophic mistake because one employee was willing to ask the questions that elected officials and public health leadership would not.
Yet losing the drug-checking program did not slow the expansion of harm reduction.
In 2018, the county’s syringe exchange had no dedicated employees and a modest budget of just over $60,000. Various employees, including Dr. Berry (Unthank), pitched in to run the program, totaling 0.51 full-time equivalent (FTE) employees for the entire year.
By 2025, the Harm Reduction Health Center employed four full-time staff and operated on a budget of $531,010 per year—roughly equivalent to the cost of four Sheriff’s deputies. At a time when residents are demanding greater public safety, that’s a significant allocation of resources toward a program that seems to expand harm.
Monthly participant encounters increased nearly fivefold, from 212 in 2023 to 975 in 2025.
Meanwhile, overdose deaths in Clallam County have more than tripled since 2018—far outpacing increases nationally, statewide, and in other states that resisted the aggressive expansion of harm reduction policies.
The pattern is difficult to ignore.
When legal concerns emerged, county leadership pressed forward.
When liability concerns emerged, county leadership pressed forward.
When common-sense objections emerged, county leadership pressed forward.
The drug-checking machine was simply the most extreme example.
In the end, Clallam County was protected not by its commissioners, not by its Health Officer, and not by the advocates determined to expand harm reduction at every opportunity.
It was protected by a lone voice willing to challenge the prevailing narrative and insist on accountability.
Clallam County needs more leaders willing to do the same.
Because when government becomes so committed to an ideology that it is willing to expose taxpayers to extraordinary risk in pursuit of it, common sense is no longer optional—it is essential.
by Ana Wolpin | May 16, 2026 | General
“In my experience, most people assume that clinical trials for childhood vaccines review safety for years, involve hundreds of thousands of children, and include a placebo control group so that outcomes in the group receiving the vaccine can be compared against the control group…
[T]he dark cold reality is that each time a childhood vaccine has been unleashed for injection into millions of children, its safety profile was, at best, unknown.”
—Aaron Siri, Vaccines Amen: The Religion of Vaccines
———————————————
What’s the Truth about Vaccines?
Part 1 of this article began an examination of statements made by Jefferson County Public Health (JCPH) in their whimsical hand-drawn quarter-page cartoon in the Port Townsend Leader shown at right.
We reviewed the 1986 National Childhood Vaccine Injury Act and the liability shield granted vaccine manufacturers which led to an explosion of the childhood vaccine schedule from a handful of shots to more than 70 doses by age 18.
We looked at Big Pharma’s capture of our regulatory agencies, the fraud and corruption in our medical establishment, and the construction of a mythology so entrenched that — like a religion — its core of zealous believers will not allow any challenges to its “safe and effective” dogma. We showed how the “Vaccines Amen” crowd, both locally and nationally, demand adherence to this gospel, denounce heretics, and impose censorship or worse on those who attempt to open up the conversation about evident dangers of vaccines.
We debunked the narrative — as asserted by public health agencies from the national Centers for Disease Control (CDC) all the way down to our local health department — that multiple injections of highly toxic concoctions are safe for our babies and children.
This article will share JCPH’s response to questions we sent them about their cartoon, including a request for sources/evidence to support their claims.
And we’ll take a look at the rise in vaccine hesitancy that likely provoked the creation of the cartoon, as well as the current battle to rein in the CDC’s bloated and dangerous childhood vaccine schedule.
First, let’s look at the facts in response to two more claims by our health department in their cartoon:
“So far, there have been no credible studies that link vaccination to chronic disease.”
and
“Vaccines are tested more than any other medicine you could give your kid.”
———————————————
Do Vaccines Cause Chronic Conditions?
“But someone told me that their kid got a chronic condition from a vaccine – what if that happens to me?”
There have been rumors that vaccines can cause:
• Autism • ADHD
• Diabetes • and more
Scientists have been researching these claims for decades. So far, there have been no credible studies that link vaccination to chronic disease.
Vaccines can actually reduce the risk of some chronic conditions, like long COVID, as well as reducing the risk of cancer from HPV and Hep B.
THE FACTS:
“I can’t think of an example where the unvaccinated child was not the healthier sibling. They typically did not develop these chronic illnesses that we’re talking about in terms of eczema and asthma and autism.”
—Elizabeth Mumper, M.D.
“What is causing the massive increase in autism and other chronic health conditions in children?
It comes down to toxins, toxins, toxins, compounded by limited nutrients that inhibit the body’s ability to detoxify. Where are these toxins coming from?
The number one source is vaccines. By injecting toxins directly into the body, you bypass the natural defense mechanisms that would normally exclude these harmful substances.
There is virtually zero autism in unvaccinated children.”
—Paul Thomas, M.D.
ARE there any credible studies that link vaccination to chronic disease? What about those pesky “rumors” that vaccines can cause autism and ADHD?
As shown in Part 1, in the 1999 CDC study comparing unvaccinated to vaccinated babies given hepatitis B shots, epidemiologist Thomas Verstraeten found increased risk not only for autism, but for sleep disorders, speech disorders, and neurodevelopmental disorders like ADHD. More than a “credible study,” it caused such panic that the CDC convened a two-day secret emergency meeting, followed by manipulation of the data to refute the link found.
Just as those findings were covered up, so have other studies been suppressed which demonstrate a link between chronic conditions and vaccines.
One obvious way to determine risk of chronic conditions from vaccines, as Verstraeten did, is to compare vaxxed versus unvaxxed children. Parents have been asking for these studies — which could easily prove or disprove vaccine-related injury and death — for thirty years.
The pat response to that request is that it would be unethical to deprive children of a vaccine in a comparative trial. That argument dissolves if one does a retrospective analysis, looking at health data already on record.
Using existing health data in a retrospective analysis is exactly what Verstraeten did.
For 35 years, the CDC collected a massive database of medical records called the Vaccine Safety Datalink (VSD). Started in 1990, the closely-guarded VSD was comprised of electronic records from 13 healthcare organizations for nine million Americans. It contained vaccination histories, health outcomes, and subject characteristics for two million children. That is the database Verstraeten was given access to in order to analyze a possible link between vaccines and neurodevelopmental disorders like autism.
“Until around 2001, the VSD was maintained at the CDC,” Aaron Siri explains. “Until that time, independent scientists who are not devout vaccine zealots were able to obtain access to the VSD at the request of members of Congress and through other legal means. The issue for the CDC is that those scientists found that vaccines cause various harms. The CDC could not have that. So the CDC moved the VSD to a health industry trade association in 2001 to avoid having the VSD data subject to FOIA [Freedom of Information Act].”
Since then, despite repeated requests, and notwithstanding the enormous database at their disposal, the CDC has refused to do further vaccinated versus unvaccinated analyses.
And in 2025 the CDC dismantled the VSD entirely. That invaluable database no longer exists. By destroying the VSD, it can never be used again for retrospective studies.
Far from our health agencies “researching these claims for decades” as stated in JCPH’s cartoon, every subterfuge available has been used to prevent that research. It has fallen to independent researchers to do the studies.
In the first peer-reviewed, published study looking at the health effects of the entire childhood vaccination schedule, in 2017 Dr. Anthony Mawson, a professor of epidemiology and biostatistics, surveyed over 600 parents of homeschooled 6- to 12-year olds. This small pilot study, including 261 completely unvaccinated children, offered a taste of other studies to come.
Mawson’s survey found that vaccinated children had 4.2 times the amount of autism and ADHD, 5.2 times greater odds for learning disabilities, nearly 20 times the rate of ear infections, and 30 times greater odds of allergic rhinitis. Unsurprisingly, pressure was put on the journal Frontiers in Public Health to retract publication of the study after it received over 80,000 online views the weekend it was released.
In 2021, Neil Z. Miller and Dr. Brian Hooker, chief science officer at Children’s Health Defense, co-authored the study “Health effects in vaccinated versus unvaccinated children, with covariates for breastfeeding status and type of birth.” Examining medical records of 1,565 children from three pediatric practices, they found vaccinated kids were:
• 5 times more likely to have autism
• 4 times more likely to have allergies
• 13.8 times more likely to have gastrointestinal issues
• 17.6 times more likely to have asthma
• 20.8 times more likely to have ADHD
• 27.8 times more likely to have chronic ear infections
An even larger study, published in 2020, looked at records from Dr. Paul Thomas’ pediatric practice in Portland, Oregon. Thomas had observed over more than three decades that the higher the vaccination rates among children he cared for, the more office visits they had for illnesses and chronic conditions. In his 2016 book The Vaccine Friendly Plan Thomas wrote that of the 15,000 children then under his care, fully unvaccinated kids were “by far, hands down, by any measure, the healthiest kids in my practice.”
He stressed that for parents who chose not to vaccinate at all, their children had the least need for medical care: “These are healthy kids. They have a robust immune system.”
The publication of his book and his outspoken stance on parents’ right to exercise informed consent on vaccination choices provoked repeated attacks on Thomas and his practice. The Oregon Medical Board demanded that he scientifically demonstrate that his alternative vaccination schedule was “as safe” as the CDC’s.
“I literally laughed,” Thomas said. “They’ve never proven anything they’ve done as safer than anything else.”
Records over a ten-year period were examined for 2,230 children who had been born into his practice, providing full health histories since birth. Working with research scientist James Lyons-Weiler in an independently verified analysis, a wide range of health outcomes were reviewed and tabulated.
As with previous studies, the results shown below confirm higher rates of chronic issues in vaccinated as compared to unvaccinated children. In all fifteen categories analyzed, the vaxxed children had significantly higher rates of conditions like asthma, eczema, and allergies; behavioral and developmental issues; and infections of all types.
In 2020, five days after publishing this robust, peer-reviewed analysis providing unequivocal proof that his unvaccinated patients were far healthier than the vaccinated children in his practice, the Oregon Medical Board issued an “emergency order” to suspend Thomas’ medical license. The pretext — he was a “threat to public health.”
After over 250,000 views online, publication of the Lyons-Weiler and Thomas paper was also retracted in a haze of vague excuses. A 2021 book The War on Informed Consent: The Persecution of Dr. Paul Thomas by the Oregon Medical Board is yet another exposé of the vaccine industry’s influence suppressing unfavorable medical research and the efforts to destroy heretics who pose a threat not to public health, but to public vaccine policy.
These and many other studies are detailed in the New York Times bestseller Vax-Unvax: Let the Science Speak. Robert F. Kennedy, Jr. and Brian Hooker compiled all the research that our health department says doesn’t exist — over one hundred studies in the peer-reviewed literature that consider vaccinated versus unvaccinated populations.
Their 2023 book, however, preceded a motherlode of vast proportions: Vax-Unvax data from the prestigious Henry Ford Health Foundation (HFHF).
In 2018, the lead researcher and head of Infectious Disease for HFHF, Dr. Marcus Zervos, took up the challenge to do a Vax-Unvax study after meeting with ICAN’s Del Bigtree and attorney Aaron Siri. A staunchly pro-vaccine doctor and proponent of mandatory vaccination, Zervos was certain that the results would demonstrate the superior health outcomes of vaccinated children.
So certain was he of what the data would reveal, he promised to publish the study regardless of the results.
HFHF’s sizable database yielded 18,468 subjects who met eligibility criteria for the study, the largest subject group yet in a Vax-Unvax analysis. Children were tracked over ten years.
Years went by before the study was finished. When all the data was analyzed, the results were not what Zervos expected. Impact of Childhood Vaccination and Long-Term Chronic Health Outcomes in Children: A Birth Cohort Study concludes:
“[I]n contrast to our expectations, we found that exposure to vaccination was independently associated with an overall 2.5-fold increase in the likelihood of developing a chronic health condition, when compared to children unexposed to vaccination.”
With results demolishing claims of vaccine safety, Zervos — who had pledged to publish them “no matter what” — reneged on his promise.
Zervos revealed on hidden camera that while the methodology and conclusions were solid, he could not face the likely repercussions if he disclosed the results:
“I think it’s a good study… but publishing something like that, I might as well retire. I’d be finished.”
He understood that challenging the medical orthodoxy would mean the end of his long and illustrious career.
Unable to convince Zervos to publish the study, Del Bigtree/ICAN tells the story in a powerful documentary, An Inconvenient Study. Released in October 2025, and winner of Best Film at the Malibu Film Festival, it is as much a tale of a medical system that demands adherence to its orthodoxy as it is a film shattering the myth that vaccines make kids healthier. Watch it here.
The Henry Ford data reinforces the consistent outcomes seen in smaller vax-unvax studies. Vaccinated children had:
• 5.6 times higher risk for neurodevelopmental disorders,
• 4.29 times more likelihood to have asthma,
• Three times higher risk for atopic diseases (like eczema),
• Nearly six times higher risk for autoimmune disorders — a category that includes over 80 different diseases,
• 2.9 times more motor disabilities,
• 4.7 times more speech disorders.
• Nearly four times more developmental delays,
• 6.6 times more acute and chronic ear infections.
Statistical comparatives were not even possible for some chronic conditions because there were zero cases in the unvaxxed cohort.
While over 600 vaccinated children in Henry Ford’s database had ADHD, diabetes, behavioral problems, learning disabilities, intellectual disabilities, tics, or other psychological disorders, out of nearly 2,000 unvaccinated children, over ten years, there wasn’t a single case of any of these chronic conditions in HFHF’s system.
And at ten years of follow-up, 57% of the vaccinated cohort had at least one chronic disorder, compared with 17% in the unvaccinated.
These studies all looked only at chronic conditions. Even more disturbing is the statistical risk of death from childhood shots. In his 2024 book Vax Facts: What to Consider Before Vaccinating at All Ages & Stages of Life, Dr. Paul Thomas compares the risk of death between vaccinated and unvaccinated children.
Government data was used to calculate the risk on each side. A summary of the methodology can be seen here.
Infants given the hepatitis B vaccine at birth were found to be three times more likely to die than those who did not get the shot. As we will see below, for 99.9% of American infants the risk of actually contracting hepatitis B is zero.
Chicken pox was considered so mild a childhood illness that when I was a kid in the 1950s parents literally held parties to spread the infection and “get it over with.” The varicella (chicken pox) vaccine was introduced in 1995 not because chicken pox was devastating children’s health — unlike vaccines, it confers lifelong immunity and helps protect against cancer later in life — but for convenience. Vaccination saved working parents the hassle of their kids being out of school for a week. The Vax Facts graphic shows children are 160 times more likely to die if given the varicella (chicken pox) vaccine than if they are unvaccinated.
And so it goes with all other routine childhood shots. Most shockingly — in sharp contrast to the conventional rhetoric about polio saving lives — the risk of death from the polio vaccine was calculated at 4,600,000 times that of not getting vaccinated against polio. Risk of death from the disease is less than one in a trillion, while risk of death from the polio vaccine is greater than 1 in 214,973.
“This is hard to believe if you haven’t heard this before,” says Thomas. “For every single vaccine on the childhood schedule, your risk of death… just looking at death because that is what parents fear the most: I don’t want my child to die of this disease for which we have a vaccine, how could I live with myself?… your risk of dying from the vaccine far exceeds your risk of dying from the disease.”
———————————————
Rigorously Tested?
“I’m just not sure vaccines are worth the risk.”
Vaccines are rigorously tested to ensure their safety. In fact – vaccines are tested more than any other medicine you could give your kid.
Children have been successfully vaccinated for generations.
THE FACTS:
“[Vaccine] testing is not long-term, not double blind, not done with proper placebos. Our children are being experimented on.”
—Brandy Vaughan, former Merck rep and founder of the Council for Vaccine Safety
“I challenge every physician and scientist to read Turtles All the Way Down: Vaccine Science and Myth and make your best effort to shoot holes in the arguments it makes. I suspect that for the vast majority it will be an eye-opening experience.”
—Mary Holland, Esq., CEO of Children’s Health Defense
Is it true that vaccines are “rigorously tested to ensure their safety”?… that “in fact – vaccines are tested more than any other medicine you could give your kid”?
The myth that vaccines are the best tested of all drugs has been repeated for so many years, it is taken for granted by the medical establishment. Anyone researching this claim soon learns, however, that like so much of the official vaccine gospel, it has no basis in reality. Just the opposite is true.
A stark comparison of vaccine testing to the testing of other pharmaceuticals can be seen at a glance in this chart from the book Vaccines, Amen:
Like the risk of death comparisons, it seems unbelievable.
Vaccine manufacturers, by law, are required to describe their clinical trials on the package insert. Far from “rigorous”, the dearth of testing for many vaccines beggars belief. While other drugs have years of testing before licensure is granted, some vaccines have been approved after safety reviews of only days.
Vaccines have the worst — not the best — safety testing protocols of any pharmaceutical product. As we reported in our 2017 study guide, “gold standard” drug testing is not applied to vaccines.
It is instructive to look once again at the package insert of the HepB vaccine Recombivax HB as an example.
Pharmaceutical drugs are required to monitor subjects for years to prove safety. Not only was the duration of the Recombivax HB trial just five days, there were only 147 infants and children who took part.
And of the 147 subjects, most were healthy babies and children up to 10 years old — not newborns, who the first shot of this vaccine is foisted upon.
Beyond being underpowered (not enough subjects), the trial had no control group. None of the subjects were given a placebo to compare outcomes with. That, too, is not permissible in drug trials. But it is the norm for vaccines.
For a clinical trial to provide meaningful safety data, several thousand subjects are needed, sometimes even tens of thousands. No pharmaceutical drug could possibly be approved with only 147 subjects after five days of monitoring and no control group.
Was there any SIDS on day 6 or 7 or 8? What about autism developing over weeks or months from a toxic load of aluminum crossing the blood-brain barrier (see Part 1)? What other long-term adverse affects might there be?
The post-marketing reports for Recombivax HB offer a glimpse of issues not seen in the 5-day clinical trial that the vaccine’s approval was based on: seizures, lupus, Guillain-Barré Syndrome (paralysis), neuropathy, multiple sclerosis, and encephalitis (brain inflammation), among many others.
The hepatitis B shot, with its 500 mcg of aluminum and residual formaldehyde, is recommended to be given within 12-24 hours of birth.
How at risk for hepatitis B is that newborn?
Requiring babies to receive three HepB shots is not only insupportable given the inadequate safety testing and post-marketing adverse reactions reported, it is especially egregious because most babies are not at ANY risk for contracting the hepatitis B virus in the first place. The virus is transmitted through sexual intercourse, dirty needles among intravenous drug users, and infection during childbirth by mothers who test positive for HepB.
Assuming a newborn isn’t having sex or sharing needles, the only possible risk is transmission from the exceedingly rare mother who tests positive for hepatitis B.
But pregnant women in the U.S. are routinely screened for hepatitis B at their first prenatal visit. Only one-tenth of one percent of pregnant women test positive for the virus: 0.1%. If a mother is not HepB positive, and the baby isn’t sexually active or a drug user, there is zero risk for that baby to contract hepatitis B.
For 99.9% of American babies, receiving a HepB injection is all risk, no benefit. And for that minuscule 0.1% who are at risk, less than 5% of those who do get infected experience permanent damage.
So why are all birthing women told their newborns need a HepB shot on the day they are born when nearly all are not at any risk? And then another shot at two months? And six months? Stories abound of hospitals threatening to call Child Protective Services (CPS) when parents refuse this day-one HepB shot.
That is the power of Pharma’s capture of the regulatory system, and of believers convinced that vaccines are always safe and effective, along with the equally pervasive mantra, “Vaccines Save Lives.”
The reality is that vaccines can take lives.
Just one example is of a family’s newborn son who died after being injected with RSV and HepB vaccines. “His parents did not want to get them but they were threatened with CPS so they complied.”
SIDS deaths reported to the CDC following vaccination is shown below for four common childhood vaccines, including hepatitis B. What was the benefit for those 410 mothers whose infants died after receiving HepB shots? How many of those babies were likely to die from the virus?
The HepB shot’s lack of safety testing is far from an outlier. Not a single vaccine on the childhood schedule has undergone the “gold standard” randomized control trial required of other drugs. None have been tested against a true placebo, which means that an accurate safety profile was never established.
Vaccine safety advocates have petitioned the CDC for proof of true placebo-based trials.
None exists.
In Vaccines, Amen, Aaron Siri shows the lack of proper controls and absence of placebo testing for every vaccine given through the first six months of life:
Much has been written about this lack of safety testing. In 2022 a group of Israeli researchers published the deepest dive yet. Along with other vaccine myths, Turtles All the Way Down: Vaccine Science and Myth, “examines in detail the institutional claims that vaccines are extremely safe and that their safety has been established by rock-solid science.”
With over 1200 references and 500+ pages, Turtles All the Way Down distills hundreds of peer-reviewed scientific papers, mainstream textbooks, the official publications of relevant government agencies, and manufacturers’ documents into an easy-to-read resource. The first part of the book is a systematic and thorough review of safety testing for every childhood vaccine.
The book’s final chapter, “The Vaccine Hoax,” summarizes their comprehensive investigation:
• Each and every one of the vaccines on the US CDC-recommended childhood schedule has been tested in clinical trials against another vaccine (or vaccine-like compound) that has a similar scope of side effects. Not a single one was tested against a true placebo, a neutral compound with no significant side effects.
• The clinical trials’ designers use this technique to cover up the high rate of adverse events expected with each new vaccine. Thus, the new vaccine can be declared “safe” and its side effects proclaimed “normal”, as the recorded side effects do not substantially exceed those of the other vaccine.
• When every new childhood vaccine is tested for safety against another vaccine, which itself was tested against another vaccine, which was tested against another vaccine, — well, you get the picture — it’s turtles all the way down.
• The use of this intentionally flawed trial methodology means that every vaccine on the US childhood schedule received FDA approval without a true measure of the actual magnitude of its adverse events.
“Current vaccine clinical trial methodology completely invalidates the claims that vaccines are safe and that they are thoroughly and rigorously tested,” they assert. “And pulling out that bogus card completely topples the childhood vaccine program’s house of cards.”
Again, the bigger question is risk-benefit.
People can accept that there may be risk from a vaccine — IF that risk is less than the risk from the disease it is targeting.
We’ve already seen the Vax Facts “Risk of Death” graph. In 2025 Physicians for Informed Consent published another analysis: Comparing 10 Disease Risks to Vaccine Risks.
It considers not just risk of death, but also risk of permanent disability. These combined risks from childhood vaccines for diphtheria, tetanus, pertussis (whooping cough), polio, haemophilus influenza type B, varicella (chicken pox), hepatitis B, measles, mumps and rubella are compared to the risk of death or permanent disability from the disease itself.
Again, in every case the vaccine has caused more death and permanent disabilities than the disease it is designed to protect against.
While JCPH’s cartoon assures us that “children have been successfully vaccinated for generations,” the truth is that chronic disease, injury and even death outweigh any benefit received through vaccination. By every metric, most children have been damaged by vaccines far more than they have benefited by avoiding the disease.
Turtles All the Way Down final chapter, “Institutionalized Fraud,” closes its exhaustive investigation into the fictitious vaccine narrative with this chilling summation:
“The magnitude of these crimes is enormous — these entities are in way too deep to ever be able to admit any wrongdoing. They will do whatever is necessary to protect the great vaccine hoax. For them it is a matter of life and death — literally.
And so it is for us.”
——————————————
Our Health Department Responds to My Inquiry
Following the publication of the health department’s cartoon, I wrote to JCPH, requesting resources for the five statements explored in these two articles:
“Can you provide sources/evidence to support these claims in the cartoon/ad (links and/or attachments)?”:
1. “Our kids face more challenges to their immune system while playing outside than they do from vaccines.”
2. “We are exposed to more aluminum by eating a tomato than from getting vaccines!” (What information can you provide comparing the danger of ingesting aluminum to that of injecting it?)
3. “The type of mercury in vaccines – ethyl mercury – is NOT harmful to us.”
4. “So far, there have been no credible studies that link vaccination to chronic disease.”
5. “Vaccines are tested more than any other medicine you could give your kid.”
I also asked:
• Who developed the content for this cartoon/ad? JCPH or an outside agency?
• Has there been a reduction in childhood vaccine uptake in the county?
I received this friendly response from Public Health Communications Specialist Alyssa Zawawi:
Hi Ana,
Thanks for reaching out to JCPH! The ad you referenced was developed by JCPH. Here are some resources that support the claims you are asking about:
1. The American Academy of Pediatrics published this article about if vaccines can overwhelm a child’s immune system and includes data about how many antigens we are exposed to in our daily lives: https://www.aap.org/en/news-room/fact-checked/fact-checked-receiving-multiple-vaccines-does-not-overwhelm-a-childs-immune-system/?srsltid=AfmBOoom-T8q459schs1FxNVIcjzDGxznf9XzLFPYMy6MmCCDAHtrR62
2. This article from the Children’s Hospital of Philadelphia’s Vaccine Education Center has information on the use of aluminum salts in vaccines and includes a section on ingesting vs injecting aluminum: https://www.chop.edu/vaccine-education-center/vaccine-safety/vaccine-ingredients/aluminum
3. The American Academy of Pediatrics writes about thimerosal (ethyl-mercury) in this article: https://www.aap.org/en/news-room/fact-checked/fact-checked-extensive-research-shows-thimerosal-is-safe/?srsltid=AfmBOoqCbGxbKslDV6IfEvk3RBKjgfvN_MgXKF4U6XIujSQyI6Is7O_X
4. Here are a few resources from the Children’s Hospital of Philadelphia that talk about vaccines and chronic disease: https://www.chop.edu/vaccine-education-center/vaccine-safety/vaccines-and-other-conditions ; https://www.chop.edu/parents-pack/parents-pack-newsletter/feature-article-do-vaccines-cause-chronic-diseases
5. This article from Johns Hopkins School of Public Health outlines the vaccine testing and approval process: https://publichealth.jhu.edu/2025/how-the-us-ensures-vaccine-safety
You can also check out Washington State Department of Health’s Immunization Dashboard (https://doh.wa.gov/data-and-statistical-reports/washington-tracking-network-wtn/immunization-data/county-public-health-measures-dashboard). This resource has a lot of information on immunization trends over time by county. For more information on vaccination rates in Jefferson County, you can also reach out to our Health Officer, Dr. Allison Berry at aberry@co.jefferson.wa.us.
Best,
Alyssa Zawawi
Public Health Communications Specialist
Jefferson County Public Health
Not surprisingly, the cartoon developed in-house by JCPH is a compilation of talking points from pharma-funded pillars of vaccine gospel.
The American Academy of Pediatrics (AAP), Children’s Hospital of Philadelphia Vaccine Education Center and Johns Hopkins School of Public Health are powerful mouthpieces for the established narrative. Their ability to deny, obfuscate and manipulate information is formidable.
We’ve already addressed numbers 4 and 5 earlier in this article. But let’s look again at the issues raised by numbers 1-3 (already touched upon in Part 1) and how the health department’s trusted sources are misleading the public.
1. “Our kids face more challenges to their immune system while playing outside than they do from vaccines.”
The American Academy of Pediatrics explains that we’re exposed in our daily lives to far more antigens (small molecules found on bacteria and viruses that elicit an immune response) than are injected through vaccination.
But the number of antigens we are exposed to is not the primary concern. The vaccines’ highly toxic formulations injected directly into the bloodstream and bypassing complex natural defenses is what is at issue (see Part 1).
Why would the AAP create this misdirect to deny vaccine damage?
Children’s Health Defense details “The Real Agenda Behind American Academy of Pediatrics: Weaponizing Children’s Mental Health and Vaccines for Profit”:
“With a budget of more than $127 million and a staff of 475, the American Academy of Pediatrics functions as a corporate and government mouthpiece that touts the wares of drug, vaccine and formula manufacturers.”
The AAP’s funding from vaccine manufacturers includes Pfizer, Moderna, Merck and Sanofi. In contrast to pediatric practices primarily helping parents navigate routine childhood illnesses as they did when I was growing up, administering vaccines is pediatricians’ bread and butter today.
Every routine “well baby” or “well child visit” from infancy throughout childhood is focused on vaccination, with more than 70 doses on the CDC schedule. Pediatric offices are dependent on this vaccine-focused approach to sustain their practices.
As disclosed by Dr. Paul Thomas, pediatricians get paid not just for the vaccine itself — financial incentives for administering vaccines include kickbacks of up to $240 per visit. Thomas estimated that by honoring informed consent and offering patients in his practice a choice, “We were losing … over a million dollars in vaccines that were refused.”
In a 2020 paper Thomas co-authored with James Lyons-Weiler, “Vaccine Practice Payment Schedules Create Perverse Incentives for Unnecessary Medical Procedures – at What Cost to Patients?”, they write it is “clear that the financial incentives to vaccinate are now a matter of survival for pediatric practices.”
“With the financial incentive to vaccinate, and to give as many as possible, it is unsurprising that many pediatric practices discharge or refuse to accept new patients who do not agree to follow the CDC recommended vaccine schedule.”
The number of pediatricians refusing to care for children who do not adhere to the full CDC schedule is considerable. A 2020 survey of AAP members published in the Journal of the American Medical Association (JAMA) revealed that half of pediatric offices report “a policy to dismiss families if they refused vaccines.”
Previous to 2018 the AAP had advised practitioners to “endeavor not to discharge” patients based on parental refusal to allow their child to be vaccinated. In 2018 that changed.
An AAP clinical report that year shifted policy guidance to support the practice of refusing care to families unless they vaccinate.
A JAMA Pediatrics opinion piece noted, “Clinicians who dismiss vaccine-refusing families seem to focus excessively on the interests of their own practice at the expense of their responsibilities to contribute to collective public health efforts.”
Despite those who argued that dismissal is ethically problematic — depriving children of pediatric care and undermining public health — the policy was rationalized as expressing “tolerance for diverse professional approaches.”
Refusing patient care supports diversity!
The AAP is so compromised that when the CDC’s Advisory Committee on Immunization Practices (ACIP) recently recommended revising the U.S. childhood vaccine schedule in line with other developed nations — changing the status of hepatitis B, rotavirus, influenza, meningococcal ACWF, hepatitis A, meningococcal B and COVID-19 vaccines from mandatory shots to a choice made jointly by parents and providers through shared clinical decision-making — the AAP sued the U.S. Department of Health and Human Services (HHS) to reverse that decision.
Despite, for example, there being no justification for a HepB shot at birth for more than 99.9% of newborns, the AAP insists that the vaccine be required for all.
“Shared clinical decision-making,” says HHS, “strengthens the doctor-patient relationship, respects informed consent, and allows recommendations to reflect individual risk — while preserving access to every vaccine.”
That shared clinical decision-making, intended to rebuild trust in public health, is anathema, however, to the AAP. Any policy that might create vaccine hesitancy cannot be tolerated. The more shots, the more the organization and its members financially benefit.
——————————————
2. “We are exposed to more aluminum by eating a tomato than from getting vaccines!”
The article from Children’s Hospital of Philadelphia supporting this statement tells us that “we are exposed to more aluminum from food than from vaccines because the exposure from food occurs daily.” It compares the amount of aluminum in foods to that in vaccines, relying on the assumption that ingested aluminum and injected aluminum are equivalent.
Concealing critical information is a typical ploy of these institutional players. Nowhere does the article reveal, as Physicians for Informed Consent explain in Part 1, that (emphasis added):
“The ATSDR [Agency for Toxic Substances and Disease Registry] oral aluminum limit is based on 0.1% of oral aluminum being absorbed into the bloodstream, as the digestive tract blocks nearly all oral aluminum (Fig. 2a). In contrast, aluminum injected intramuscularly bypasses the digestive tract, and 100% of aluminum may be absorbed into the bloodstream over time (i.e.,the proportion of absorbed aluminum is 1,000 times greater).
This Children’s Hospital of Philadelphia article was “reviewed by Paul A. Offit, MD.”
That helps explain the article’s deception by omission. Offit is the industry’s top “medical expert” propagandist, popularizing such lies as vaccines are the best tested of all products, far better than pharmaceuticals. The inventor of a rotavirus vaccine, with a $1.5 million research chair funded by Merck at Children’s Hospital, he is one of pharma’s most aggressive proponents for mandatory vaccination.
Among Offit’s many outrageous assertions is that vaccines are safer than vitamins. He is infamous for his statement that healthy infants could safely get up to 10,000 vaccines at once. He later upped that figure: “I would say you probably could get 100,000 vaccines every day.”
——————————————
3. The type of mercury in vaccines – ethyl mercury – is NOT harmful to us.”
The AAP article linked by JCPH to make this assertion is riddled with misinformation about the dangerous neurotoxin ethylmercury (thimerosal) in vaccines.
“AAP’s assessment of the best available evidence has always been, and continues to be, that thimerosal is a safe additive in appropriate amounts.”
A blatant rewriting of history, this has not “always been” AAP’s assessment. Prior to being completely subsumed by Big Pharma, in 1999 the American Academy of Pediatrics recognized the risk from and called for the immediate removal of thimerosal from infant vaccines.
Now the AAP is claiming they only called for thimerosal’s removal because the public mistakenly believed mercury in vaccines was dangerous and they wanted to make parents feel better about vaccinating their kids.
The AAP knew then and surely knows today that contents of unused thimerosal-containing vaccine vials are required to be disposed of as federally hazardous waste. What they are now calling “appropriate amounts” in thimerosal-preserved vaccines is literally 250 times the level classified as a toxic hazardous waste by the EPA. (See Part 1)
Proof that thimerosal is safe, they tell us, is that “autism rates actually rose after thimerosal was removed from childhood vaccines.” As we detailed in Part 1, toxic aluminum replaced the toxic mercury when thimerosal was removed from most (not all) childhood vaccines. Additionally, the number of doses on the childhood vaccine schedule nearly tripled. Of course autism rates rose.
In addition to the AAP lying about it’s past position on thimerosal in vaccines, again we see misinformation by omission.
No doubt the well-meaning folks at our health department believe and rely on this institutional fiction. But as more people are becoming informed, the vaccine religion’s foundations are wobbling.
——————————————
Vaccine Hesitancy On the Rise
and the Battle to Maintain Control of the Narrative
“I think we’re finding that a lot of the parents are informing themselves, and are less malleable in the office setting, because with the information age that we’re in, this information is available that wasn’t available before the doctor was the only source of information. You didn’t have any way to look it up. And now, people do. So, this may be a problem that extends into the future.”
—Dr. Joe Wiley, Lewis County Health Director
The young boy in JCPH’s cartoon has heard “rumors” that vaccines can cause chronic conditions like autism and asks, “What if that happens to me?”
The girl in the cartoon wonders if getting vaccines is “worth the risk.”
Despite the relentless barrage of safe and effective messaging, public health is now faced with the problem of parents accessing information beyond their doctors’ offices. Now capable of “informing themselves,” they are “less malleable” (manipulable).
As suspected, in line with the national trend, childhood vaccine uptake has been dropping in Jefferson County.
Looking at the Washington Department of Health Immunization Dashboard, a steady reduction in childhood vaccination rates following the not-so “safe and effective” COVID-19 injection fiasco is evident. For example, the HepB vaccine dose given at birth shows 72.8% uptake in 2022, declining to 53% in 2025.
Every county in the state shows the same trend.
Similarly, the dashboard shows drops in vaccine uptake for 19- to 35-month-olds in Jefferson County between 2021 and 2025 for these shots:
In Informed Choice Washington‘s March 18 newsletter, Gerald Braude covered a presentation given by former pediatrician and current Lewis County Health Director Dr. Joe Wiley to their Board of Health. The quote above describing the problem of parents being less “malleable” because they can now access their own information is from that presentation.
Wiley linked the precipitous drop in vaccination rates in Lewis County to multiple factors in this slide:
In his follow-up comments, he expanded:
“Not mentioned here, but some have noted that the pharmaceutical companies provide lots of funding… Lots of funding for medical journals and medical organizations make consumers suspicious. Some have also found that the National Childhood Vaccine Injury Act of 1986 as suspicious because it exempts the pharmaceutical companies that make the vaccines exempt from liability should anyone be injured from the vaccine. And they fear that the pharmaceutical companies that are making the vaccines may take shortcuts because they don’t have to worry about liability.”
Much of his additional commentary focused on the COVID-19 debacle eroding public trust in vaccines.
“There’s a lot of lost trust among the population,” Wiley said. “The medical offices see it, I hear it from them, and you’ve probably seen it in your family, even, if not within yourself. And it seems like the available data that we’ve looked at here supports that vaccine hesitancy.”
While acknowledging that the available data supports vaccine hesitancy, public health agencies nonetheless see that as a problem. They persist in gaslighting us with assurances that mercury and aluminum in vaccines is perfectly safe, that vaccines are more rigorously tested than any other drugs, and that they do not cause chronic health conditions — all patently false assertions.
In Jefferson County, we continue to face censorship and dismissal when challenging that gaslighting.
Right after JCPH’s cartoon was published, the Port Townsend Leader rejected a letter to the editor directly responding to its claim about safety testing. The writer who submitted it described failure of government oversight in which a 1986 law mandating reports from a vaccine safety task force had been been ignored for forty years. The task force had never fulfilled its mandate and Congress never received a single biennial report on vaccine safety improvements that the law required. The Leader censored that information.
NextDoor also censored a conversation about our previous article, Part 1. A Free Press reader posted a link to the article. That elicited several comments of appreciation, agreeing with its content… but those were quickly overshadowed by a few people who then dominated the comments proclaiming that the information presented was false. No supposed inaccuracies were ever cited; the commenters just attacked the Free Press and its writers. The post was deleted soon after as “misinformation”.
At the monthly County Public Health Report broadcast on KPTZ on May 4, a listener asked Health Officer Dr. Allison Berry for a response to our article. Rather than address any of the substance, she, too, just used the convenient, dismissive “misinformation” label. No rebuttal of a single inaccuracy, just a long generalized diatribe about identifying misinformation online. That may be addressed in a separate follow-up article.
——————————————
On a national level, the stakes are far higher. The struggle to maintain control of the vaccine narrative has expanded from the kind of censorship and dismissal we are subject to locally to an intense legal battle in federal court.
As previously discussed, the American Academy of Pediatrics (AAP) and other organizations have sued HHS to prevent “shared clinical decision-making” on any of the childhood vaccines. For doctors and other health advisors to have honest conversations that acknowledge potential risks would increase vaccine hesitancy.
They have also targeted the CDC’s Advisory Committee for Immunization Practices (ACIP) which makes recommendations for vaccines on the childhood schedule.
Historically, ACIP had been comprised entirely of members with financial ties to pharma. All committee members had conflicts of interest, rubber-stamping every vaccine that came to them for approval.
A 2000 Committee on Government Reform report concluded:
“The CDC routinely grants waivers from conflict of interest rules to every member of its advisory committee… Four out of eight CDC advisory committee members who voted to approve guidelines for the rotavirus vaccine in June 1998 had financial ties to pharmaceutical companies that were developing different versions of the vaccine.”
Dr. Paul Offit from Children’s Hospital of Philadelphia, for example, was an ACIP member cited for conflict of interest in a hearing held by the Committee on Government Reform. As one of the rotavirus vaccine developers funded by pharmaceutical companies, he “voted on three rotavirus issues, including making the recommendation of adding the rotavirus vaccine to the Vaccines for Children program.” Getting that vaccine on the schedule earned Offit millions of dollars.
One of Robert Kennedy Jr’s first acts as new HHS Secretary was to replace the pharma-centric ACIP members with a balanced group of medical experts without conflicts of interest. It is that independent group which made the recommendation for shared decision-making that the AAP is opposing.
The new ACIP panel also recommended removing mercury from flu vaccines. And they voted to end the universal recommendation that all newborns receive the hepatitis B vaccine within 12-24 hours of birth. All those long-overdue recommendations were designed to restore trust in public health.
The AAP and other pharma-funded organizations have sued to reverse all those decisions.
And within hours of ACIP voting to discontinue the hepatitis B shot requirement for babies born to HepB-negative mothers, the West Coast Health Alliance (California, Oregon, Washington, and Hawaii) announced they, too, would reject the recommendation and continue promoting the automatic hepatitis B birth-dose.
In a final attack, the AAP’s lawsuit sought disbandment of ACIP.
In March, a U.S. District Judge issued a stay on all counts, which put a pause on all new ACIP recommendations and prevented the committee from continuing to meet. The judge did not issue the injunctions AAP sought to permanently block ACIP’s efforts, but that is still possible.
The ruling has been appealed, both by HHS and separately by the nonprofit Children’s Health Defense (CHD). Those appeals are pending.
In a counter-measure in January, CHD and five other plaintiffs sued the AAP, accusing it of running a decades-long racketeering scheme to defraud the public about the safety of the CDC’s childhood vaccination schedule.
The lawsuit alleges that the AAP:
• Promotes vaccine safety claims without comprehensive safety testing, including the absence of studies comparing health outcomes in vaccinated and unvaccinated children
• Suppresses and misrepresents scientific uncertainty, creating a “false certainty”
• Relies on a foundational fraud, a theoretical claim that infants could safely receive thousands of vaccines at once, despite no clinical evidence of the safety of that claim
• Uses its influence to punish dissenting physicians, damaging the careers of pediatricians who questioned vaccine safety claims
• Fails to disclose financial relationships with pharmaceutical companies that manufacture childhood vaccines
Among the plaintiffs are physicians whose professional reputations were harmed for opposing AAP’s guidelines, and the parents of four children who died or were injured after receiving routine childhood vaccinations. Dr. Kenneth Stoller, who lost his medical license in California and New Mexico after he granted medical exemptions to vaccine mandates, said “AAP turned pediatricians into vaccine delivery systems and destroyed the ones who asked questions.”
On April 3, AAP filed a motion to dismiss the RICO case; plaintiffs’ response is due on or before June 9.
This is the legal battle in play.
——————————————
Meanwhile, in the court of public opinion, increasing vaccine hesitancy shows that the pharma-medical complex is losing its stranglehold.
As public trust erodes, the AAP and other pharma-funded groups reveal their desperation — suing to continue HepB vaccination of newborns who have zero risk, trying to block shared clinical decision-making between parents and providers, fighting to keep neurotoxic mercury in the flu shot.
These are the institutions and organizations Jefferson County Public Health relies on for its messaging to our community. Given their denial of vaccine dangers in this recent cartoon, does our health department agree with the AAP’s efforts to prevent shared clinical decision-making, remove mercury from vaccines and force HepB shots on all newborns?
What is their position on pediatricians who refuse care to children whose parents decline vaccinations?
Those might be good questions for Health Officer Berry at her next public health update.
——————————————
by Ana Wolpin | Apr 12, 2026 | General
“According to the CDC and public health authorities, parents who choose not to vaccinate their children are typically highly educated. CDC data reflect that half of American school children are not fully vaccinated, and at least 1 in 88 toddlers are completely unvaccinated. Why would the parents of these children, comprising a large part of the nation’s brain trust, choose not to vaccinate their children?”
— Aaron Siri, from the foreword of “Vaccines, Amen: The Religion of Vaccines”
———————————————
“What’s the Truth about Vaccines?” asked Jefferson County Public Health (JCPH) in a quarter-page ad in the March 11 Port Townsend Leader. The hand-drawn, whimsical cartoon-style presentation and the ad’s content offered a light-hearted attempt to ease parents’ concerns about vaccinating their children.
“This is a JUDGEMENT FREE guide to learn about vaccines,” the ad opens with. “You don’t need to have your mind made up to start reading. BRING YOUR CURIOSITY!”
Among the statements made:
• “Our kids face more challenges to their immune system while playing outside than they do from vaccines.”
• “We are exposed to more aluminum by eating a tomato than from getting vaccines!”
• “The type of mercury in vaccines – ethylmercury – is NOT harmful to us.”
• “So far, there have been no credible studies that link vaccination to chronic disease.”
• “Vaccines are tested more than any other medicine you could give your kid.”
The health department’s ad comes at a time when childhood vaccination rates are dropping steadily across the country. Along with reduction in vaccine uptake, there is also a rise in the rate of parents seeking vaccine exemptions for their children.
In Part 1 of this article, we will explore the growing awareness causing this shift, share some local history on attempts to open up the conversation about vaccines in our community, and examine some of the statements above that our health department has made to reassure parents that they needn’t worry about common vaccination concerns.
Three Distinct Attitudes About Vaccination
Aaron Siri, quoted at the top of this article, is managing partner of the highest profile law firm handling vaccine-related cases in the U.S. Over the last decade he has deposed the world’s leading vaccinologists, challenged medical mandates, and won awards for vaccine injury cases. He has prosecuted over a hundred lawsuits against health agencies, successfully suing the FDA to release Pfizer and Moderna’s Covid-19 vaccine licensure documents, winning many cases restoring medical exemptions including for the U.S. military, and forcing transparency when the CDC refused to release hidden V-safe data tracking adverse reactions to the Covid-19 shots.
In this pursuit, Siri describes experiencing three categories of people:
• Parents who do not vaccinate. Parents who choose to forego vaccines, he says, are not only highly educated, but “often scientifically literate. Many are medical professionals. Leading scientists.” He quotes vaccine promoter Emily Brunson, PhD, who acknowledges: “When you look at hesitancy in the U.S., the group who is most likely to purposefully choose to not vaccinate are highly educated. In speaking with them, these are people who have read the primary literature themselves, and they’re correctly interpreting it.”
• Parents who do vaccinate. Almost all “have never really thought much about these products… they just go with the flow,” says Siri. “They often do what the media says good parents are expected to do—trust their doctors.” They are, however, open-minded and able to process new information. He finds that their “views are susceptible to change upon presentation of actual evidence.”
• The “Vaccines Amen” crowd. For these believers, the story that vaccines are a modern medical miracle — safe and effective! — is a sacred cow. “This is the group of parents, doctors and public health professionals—a small army of them—who have a fervent belief in vaccines,” says Siri. “When these beliefs are challenged, this crowd gets angry.”
Unable to “accept even official government data showing that many of their core beliefs regarding vaccines are false,” these zealots are incurious and entrenched. Their fanaticism is faith-based, akin to religious zealotry.
“They regurgitate canned answers they have never researched—essentially mantras,” says Siri. At their most extreme, “for those who refuse to adopt their beliefs, they demand that the refusers be censored, have their rights taken away, and be mandated to be injected.”
As this article will show, the claims made in our health department’s ad repeat medical dogma that has persisted for decades with no basis in reality. At best the narrative is a wishful fairy tale. At worst it is dangerous disinformation.
As Siri expresses, “I think most pediatricians, doctors and public health authorities mean well. They believe they are engaging in God’s work. And that is often the problem that makes them blind to reality.”
Is our health department simply “going with the flow,” unaware that the claims made in their ad are mythology? Or are they so entrenched in their fervent belief in the vaccine narrative that they cannot consider information that disproves the gospel?
‘Vaccines Amen’ Bullies and Gatekeepers in Jefferson County
In 2016, a documentary film disclosing a decade-long CDC cover-up created an uproar in the news, sparking a long-overdue national conversation. Senior CDC scientist turned whistleblower William Thompson revealed privately in 2014 that data linking the MMR vaccine (measles/mumps/rubella) to autism had been manipulated by the agency ten years earlier.
When top CDC officials learned that their 2004 study results showed a dramatic increase in autism after MMR vaccinations, they’d ordered Thompson and other scientists to destroy all evidence. The agency then had the research team revise the study parameters and manipulate the data to disprove a link. Ultimately, the only way they could eliminate the evident risk was to eliminate from the study the groups of children most likely to regress into autism following their shot. The fraudulent, re-worked study was then released to declare that it had proven MMR vaccines did not cause autism.
Believing the order to destroy data was illegal, Thompson secretly saved over 10,000 pages of documents. He would reveal them a decade later, conscience-stricken over the likely damage in ongoing vaccine injury the cover-up was causing.
The CDC had conducted the study in response to petitions from over 5,000 parents in vaccine court who had witnessed their children regress into autism from the MMR shot. When the fraudulent “results” were released, those petitions were dismissed with the stroke of a pen. The CDC announced: No more research money will be spent on this question; “the science is settled.”
This fraud was the subject of the shocking and controversial movie Vaxxed: From Cover-Up to Catastrophe.
Scheduled to premier at the Tribeca Film Festival, Big Pharma pressure forced its cancellation. The effort to suppress the film only gave it more publicity and heightened public interest. Screenings across the country opened a floodgate. A tsunami of parents started speaking out about their own children’s vaccine injuries.
Working with the film’s distributor and Rose Theatre owner Rocky Friedman, Annette Huenke (now a PTFP co-editor) set up a screening of Vaxxed in Port Townsend. A January 2017 date was set and Huenke wrote the theater a check as a deposit for the screening. Posters were printed and tickets went on sale, posted on the Rose Theatre’s Facebook page.
Within 24 hours of the film being announced, the screening which had been planned over months was canceled.
Both the Facebook post announcing the film screening and a comment it had generated were quickly pulled from the page. Owen Rowe, then director of the now-defunct Jefferson Community School and board member of the Food Co-op (he is currently a Port Townsend city councilman), was outraged that the theater would dare to screen that “fraudulent film” which he undoubtably had not seen. Before the post was deleted Huenke was alerted to the angry tirade shaming Friedman on the theater’s Facebook page.
In an apologetic exchange that Friedman had with Huenke after canceling the film, he said,
“I am very sorry that I caved to this and didn’t stand up to it. It was not pleasant for me or for the business that I’ve created. Actually, it was far worse than the death threat that I received when I was intending to show a movie by Michael Moore a long time ago… Please let me reimburse you for whatever expenses you have incurred – posters or other advertising.”
Far worse than a death threat?!
Self-appointed community gatekeeper Owen Rowe demonstrated the epitome of the angry zealotry that Siri describes. By threatening Friedman and the Rose Theatre, he’d eliminated the heinous possibility of people being exposed to information that challenged his beliefs — effectively demanding censorship to squelch independent thinking.
People Who Do the Research
Following that dramatic attack and cancellation, I joined a group of local folks concerned about censorship. We formed a vaccine study group that dove into the vaccination question with a great deal of curiosity. We met every week for the better part of a year to discuss books, films and other materials that were challenging the dominant “vaccines are a modern medical miracle” story.
The first shock for anyone just beginning this research was learning about the 1986 National Childhood Vaccine Injury Act.
In the 1980s, pharmaceutical companies were losing so much money settling lawsuits for vaccine injury (predominantly from the DPT shot – diphtheria/pertussis/tetanus) that the industry threatened to stop making vaccines unless the government shielded them from damages. Bowing to the pressure, in 1986 Congress removed all liability from drug companies for childhood vaccines they produced. This get-out-of-jail-free card, eliminating industry responsibility for safety, was unprecedented.
The 1986 act set the stage for the breathtaking industry capture, government cover-ups and bombardment of “safe and effective” messaging that followed.
With vaccine makers now absolved of all medical and legal liability when children die, become chronically ill with vaccine-induced disorders, or are otherwise disabled from vaccine injuries, pharma had a field day. Vaccines became Big Pharma’s most profitable product division almost overnight.
Not only did profits skyrocket because pharma was shielded from damages, they were guaranteed sales with zero marketing costs. Each new childhood shot approved was automatically added to the CDC’s Childhood Vaccine Schedule, with the assurance that tens of millions of children would receive them at routine pediatric visits. The CDC partnered with pharma as the primary purchaser, distributor and promoter of billions of dollars of vaccines annually.
A more-is-better free-for-all ensued.
While children had received just five vaccine doses in three shots in the 1950s and ’60s when I was growing up (none during pregnancy or in the first 12 months of life), by 1986 children were receiving 25 doses/12 shots. In the decades following the 1986 act the childhood schedule exploded to 73 doses/54 shots.
New vaccines were developed for illnesses like hepatitis B and rotavirus, for which there was little risk and which effectively had 100% survival rates for healthy American children. Mild illnesses which formerly helped strengthen developing infants’ and children’s immune systems were now vaccinated against, all fodder for pharma’s liability-free cash cow.
Pregnant mothers were injected, infants started receiving shots on their first day of life, and the practice of administering multiple shots — as many as ten doses in eight shots at one time (never tested in combination) in a euphemistically labeled “Well Child Visit” — became routine.
In my childhood years, autism, peanut allergies, ADHD, asthma, and other issues common among children today were virtually nonexistent. Back in the 1950s and ’60s we had some of the world’s healthiest children. It was a rude awakening, especially for those of us in the Baby Boomer generation, to learn that the chronic illness rate in U.S. children which had been negligible when we were kids had jumped to 12.8% in the 1980s, then to 54% by 2011.
More than one in two American children in the 2011 survey had a diagnosed chronic health condition such as an autoimmune disorder, diabetes or obesity, a neurodevelopmental disorder, or a mood or behavioral disorder. Today the percentage is surely even higher, but updated statistics are not available.
During my childhood we had one of the best infant mortality rates in the world. But after embarking on the world’s most aggressive vaccination program, the U.S. had twice as many first-day infant deaths as all 27 EU nations combined. An analysis of two decades of U.S. data (1990-2010) showed that infants who received the most vaccines had the worst hospitalization and death rates. And a 2011 study of data from 34 developed nations found that countries giving the least vaccines had the lowest infant mortality. [source]
With passage of the 1986 act, febrile seizures after vaccination, SIDS, autism, learning disabilities, food allergies and other chronic illnesses became normalized. Today the percentage of children carrying epipens, needing inhalers, and/or taking Ritalin, amphetamines and antidepressants is staggering.
Was the rise in all these chronic diseases and even deaths a direct result of the parallel exploding vaccination program? Did correlation equal causation?
Following the release of the film Vaxxed, parents came out of the woodwork wanting to share their stories of vaccine injury. The Vaxxed bus was born. Traveling to every U.S. state on the continent, its dedicated team video-taped thousands of stories of vaccine injury and death. More than 8,000 names were signed on the bus’ exterior of adults and children injured or killed by vaccines.
The common themes in stories parents recounted were eerie. Many described rushing their infants or toddlers to the ER with convulsions, 105° fevers, horrifying screams and seizures after their shots, only to be told this is normal… we see this all the time… it has nothing to do with the vaccines. In some cases, their children shut down immediately following the shots, stopped making eye contact, lost verbal communication. Others regressed more slowly into autism.
The worst were the SIDS (Sudden Infant Death Syndrome) cases. Some within hours of getting vaccinated, and nearly all within a week of their “Well Baby” shots, would be found dead in their cribs after being put down for a nap. More on that below.
The HighWire was also launched around that period, hosted by Del Bigtree who had produced Vaxxed. A weekly podcast “dedicated to investigating our food, our air, our water, our drugs and our vaccines, with the mission of identifying and stopping the spread of man-made disease,” it is the media adjunct to the nonprofit Informed Consent Action Network (ICAN) which is responsible for many of the legal actions described earlier.
Along with Vaxxed, other films and videos informed our discussion. Trace Amounts, explored the link between the mercury-based preservative thimerosal and autism. The documentary series The Truth About Vaccines covered a wide range of issues, and continues to provide up-to-date information about news in this field.
Several groundbreaking books were also published. Among the most important:
Our group learned about the suppressed 1999 study linking thimerosal in vaccines to neurodevelopmental disorders and to the exponentially-increasing autism rates, which as in the MMR/autism study, resulted in the CDC secretly reworking the data to cover up the association. It was a strategy we would see employed whenever findings challenged the “safe and effective” narrative.
We became aware of other toxic ingredients in vaccines as well as serious issues regarding safety testing. A further revelation involved suppressed studies comparing vaccinated children to unvaccinated.
These, along with more recent developments, will be expanded on below and in Part 2, with the examination of JCPH’s claims.
At the same time that decades of fraud, false narratives and industry capture were being exposed, the pharma-medical-industrial complex was aggressively pushing to eliminate all challenges to the vaccine narrative.
Pharma-funded politicians were advancing legislation to remove people’s religious and personal medical vaccine exemptions, and to deny children who were out of compliance with the CDC schedule access to public schools. We saw doctors and scientists who raised concerns about vaccine dangers get persecuted with a vengeance by the industry-controlled medical establishment. Any MD challenging the safe and effective narrative — even just for authorizing vaccine exemptions for patients — was attacked, marginalized, and in some cases lost their licenses.
By the time our vaccine study group wrapped up our research, over one hundred legislative bills were pending to eradicate vaccination choice in forty states, foreshadowing the Covid insanity to come.
Our group considered ways to broaden the conversation locally. We decided:
1) to seek another venue to host a screening of Vaxxed, and
2) to develop a study guide to share our research more broadly.
Given the sacred cow nature of the vaccine narrative, and the Rose Theatre experience, we knew there would be resistance.
What we got was full-blown censorship.
The Next Round of Gatekeeping and Censorship
The Uptown Theater was going through renovations and closed during this time period, so there was no possibility of Vaxxed showing there. But in addition to theater runs, viewings of the film were happening in gatherings all over the U.S. through an organization called Gathr. We reached out to local churches in an effort to find an alternative venue.
There, too, we were met with refusals. Not even the Unity Church or Quimper Unitarian would allow the film to be shown.
Over a period of several months our group developed a vaccine study guide — VACCINATION: Where there is Risk, there must be Choice. The guide summarized basic information being suppressed, providing an overview and starting point for anyone interested in researching the subject for themselves.
We created a print version of the guide, and working with the Port Townsend Leader’s advertising manager, arranged to pay for its inclusion as an insert in the newspaper. We were told that as long as our information was credibly sourced and could be confirmed through Google Scholar, it would be acceptable.
Everything in the guide was meticulously documented — including CDC links, National Library of Medicine studies, and vaccine package inserts — all substantiated through Google Scholar. However when Publisher Lloyd Mullen was given a copy, his note of rejection was swift:
“Unfortunately, we will not be able to print or insert your flyer in our newspaper.
The reason: correlation does not imply causation.”
Once again, allowing people to consider varied perspectives and then make up their own minds was not permitted. Mullen, representing democracy’s supposed Fourth Estate, was our community’s ultimate gatekeeper. This censorship was applied even when we submitted letters to the editor about vaccines. Our opinions, if they challenged local health authorities, were not allowed on the OPINION page.
Stephen Schumacher (also a PTFP co-editor now) would experience the same censorship several years later regarding the experimental mRNA Covid vaccines. First the Leader refused to print his and other community members’ letters to the editor if they challenged public health’s Covid messaging. Then, when Schumacher attempted to pay for ad space, that, too, was censored — a “business decision” he was told (see Of Covid Testing, “Misinformation” and Censorship).
An online version of our study guide is still posted. It contains even more information than the print guide did, with over 150 links to information and resources — articles, studies, videos and data. Many links, like youtube videos, have since been scrubbed, but current sources are linked throughout this article.
While the material covered in our 2017 guide thoroughly debunked the old talking points still being trotted out today by Jefferson County Public Health, nine years later the research is even more damning.
The devastating Covid psy-op perpetrated on a trusting public shook up many health professionals, causing them to question what other lies they’d been fed. Once they started digging into the larger vaccine narrative, the depth of betrayal in what they’d been trained to accept as gospel was profound.
As John Leake and renowned cardiologist Dr. Peter McCullough explained in their 2025 book “Vaccines Mythology, Ideology, and Reality”:
“Prior to 2020, we had never questioned the sacred cow of vaccines. It was only in 2020, when we observed the stupendous chicanery of the COVID-19 rollout, that we began to wonder about the entire vaccine enterprise. Since then we have methodically studied the literature on vaccination…”
Investigations by formerly pro-vax doctors, scientists and researchers who had never considered questioning vaccine gospel have generated a whole new wave of exposés. Some of the information shared below is from new voices like these.
The health department asked that you BRING YOUR CURIOSITY.
We invite them to do likewise.
Again quoting Aaron Siri’s forward in Vaccines, Amen:
“You are about to learn things you can never unlearn.”
Examining Public Health’s “Truths” About Vaccines
Let’s now consider the claims in Jefferson County Public Health’s ad. Following each cartoon panel’s question and our health department’s answers are the facts.
Immune System Challenges?
“I heard that giving too many vaccines at a time can overwhelm my kid’s immune system.”
It’s natural to be worried about how much our kids can handle. The truth is, a child’s immune system can handle a lot!
Our kids face more challenges to their immune system while playing outside than they do from vaccines.
THE FACTS:
“Prior to the introduction of organized vaccination programs, ‘crib death’ was so rare that it was not mentioned in infant mortality statistics… By 1972, SIDS had become the leading cause of post-neonatal mortality (infant deaths occurring between 28 days and 1 year of life) in the United States.”
— Neil Z. Miller,
“Vaccines and sudden infant death: An analysis of the VAERS database 1990–2019 and review of the medical literature”
The death of any child is tragic. The sudden death of a formerly-thriving child is shocking. It was not until mass vaccination that the term SIDS — Sudden Infant Death Syndrome — even existed. SIDS is the most extreme example of how vaccines can sometimes overwhelm a child’s immune system.
Does correlation imply causation? Historically, parents had not been finding healthy babies unexpectedly dead in their cribs hours after “playing outside.” But that was the experience of some parents following vaccination.
As Neil Z. Miller observes above, following the introduction of national vaccination programs in the U.S., SIDS became the leading cause of infant mortality.
Like other dangers associated with vaccination, health authorities sought to explain away this new phenomenon. In his 2021 report “Vaccines and sudden infant death: An analysis of the VAERS database 1990–2019 and review of the medical literature,” Miller explains:
“Throughout the 1980s, sudden infant deaths continued to skyrocket. Parental concerns about an apparent link between childhood vaccines and SIDS reached a fever pitch. Many parents were afraid to vaccinate their babies. Authorities sought to reassure parents that vaccines are safe and claimed that sudden unexplained infant deaths (SUID) following vaccines were merely coincidental.”
New diagnoses were concocted, and sudden deaths were reclassified, a common strategy used by health authorities to obscure associations with vaccine damage. Even infants who showed extreme distress following injection — screaming, having seizures, collapsing, then dying within hours of their shots — were not classified as vaccine-induced deaths.
In a “Back to Sleep” campaign, parents were told that their babies’ sleeping position was the culprit — that they needed to be laid on their backs, not face down. In some cases, parents were subjected to investigations for child abuse, blaming their child’s sudden death on another new phenomenon, Shaken Baby Syndrome. Adverse reactions commonly seen after vaccination — extreme irritability, lethargy, poor feeding, breathing problems, convulsions, vomiting, and pale or bluish skin — were identified as symptoms resulting from parents violently shaking their babies.
Miller analyzed 2,605 deaths reported to the Vaccine Adverse Events Reporting System (VAERS) between 1990 and 2019. Of these, 17% of deaths occurred on the day of vaccination and 48 percent within two days. A full 78.3 percent occurred within seven days post-vaccination. All coincidences?
So how do impacts from vaccines being injected in children compare to environmental exposures they face when “playing outside”?
Humans have evolved for millennia playing in the dirt and being exposed to pathogens in the environment. The immune challenges a child faces in nature are met by a series of complex defenses. Four layers of the immune system come into play: skin, mucous membranes, lymphatic and blood.
As described by Thomas Cowan, MD, in “Vaccines, Autoimmunity, and the Changing Nature of Childhood Illness“:
“When we are healthy, enzymes in the mouth, acid in the stomach, and microbes in the lower gut will often destroy pathogens. If a pathogen escapes these first lines of digestive defense, then the villi will prevent their access to the bloodstream. If the villi are compromised, we have the physical barrier of the smooth muscular layer of the intestinal wall. In health, these systems function together to screen pathogens from the bloodstream. They are, in essence, guardians of our health.”
An intramuscular injection bypasses all these intricate protective mechanisms, sending the needle’s contents directly into the bloodstream. And often across the blood-brain barrier as well.
Looking at how vaccines can cause sudden infant death, Miller notes that “several theories regarding the pathogenic mechanism behind these fatal events have been proposed.” They include:
• inflammatory cytokines;
• toxic adjuvants (such as aluminum) that cross the blood-brain barrier; and
• biochemical or synergistic toxicity due to multiple vaccines administered concurrently.
This graphic illustrates one of these mechanisms — how toxic adjuvants (in this case aluminum) are transported by macrophages across the blood-brain barrier (BBB).
If a single vaccine can cause SIDS in a small percentage of babies, how many children might have damage on a lesser scale from the dozens of shots received in just the first year of life? Typically a “Well Baby Visit” consists of numerous vaccines all administered on the same day.
Parents are rightly concerned that multiple shots in one visit compounds the risk. As many as ten doses given in eight shots are now routine in pediatric practices.
An example is the six month “Well Baby Visit.” The CDC schedule calls for 6-month-olds to be injected with DTaP (diphtheria/tetanus/pertussis), Hib (haemophilus influenza type B), HepB (hepatitis B), PCV (pneumococcal), IPV (polio), Influenza (seasonal flu), Rotavirus, and COVID-19 vaccines.
As shown in this guide, those administering the vaccines are instructed on how to inject multiple shots into every limb.
It is true that “a child’s immune system can handle a lot”…
…but injecting the toxic load of a vaccine directly into a developing infant’s bloodstream, bypassing the body’s layered natural defenses, cannot even begin to compare to natural processes engaged when “playing outside.”
———————————————
Dangerous Chemicals in Vaccines?
“Aren’t there DANGEROUS chemicals in vaccines?
Are they even safe?”
Let’s take a look at some ingredients that can make folks nervous:
[1] ALUMINUM
Aluminum occurs naturally in the air, water and soil.
We are exposed to more aluminum by eating a tomato than from getting vaccines!
THE FACTS / ALUMINUM:
“Our calculations show that the levels of aluminum suggested by the currently used limits place infants at risk of acute, repeated, and possibly chronic exposures of toxic levels of aluminum in modern vaccine schedules.”
—James Lyons-Weiler and Robert Ricketson,
“Reconsideration of the immunotherapeutic pediatric safe dose levels of aluminum”
Folks SHOULD be nervous about aluminum being used in vaccines. Just because it “occurs naturally” does not mean a substance is safe. While aluminum is the most abundant metal in the earth’s crust, it is tightly bound with other elements like silica, and not bioavailable. It has no physiological role in the body, and whether ingested, inhaled or injected, isolated aluminum is toxic.
Eating or drinking aluminum can be harmful, but both the digestive system and the liver are able to filter it before it reaches the bloodstream, affording some degree of protection. Injecting aluminum through a vaccination bypasses these protections, placing it directly into the bloodstream.
Regarding the aluminum in that tomato, according to Physicians for Informed Consent:
“The ATSDR [Agency for Toxic Substances and Disease Registry] oral aluminum limit is based on 0.1% of oral aluminum being absorbed into the bloodstream, as the digestive tract blocks nearly all oral aluminum (Fig. 2a). In contrast, aluminum injected intramuscularly bypasses the digestive tract, and 100% of aluminum may be absorbed into the bloodstream over time (i.e.,the proportion of absorbed aluminum is 1,000 times greater).” [source]
Aluminum is used in many childhood vaccines like HepB as an adjuvant, to provoke an immune response. It is known to cause brain damage at all doses. Aluminum poisoning has been linked to autism, SIDs, seizures, autoimmune issues, Alzheimers, neurological damage, impaired renal function, demyelinating disorders such as MS, and cancer. [source]
In the mid-1900s, the FDA established a maximum limit of 850 mcg (0.85 mg) of aluminum per vaccine dose. Then, based on a 1997 study of preterm infants receiving intravenous-feeding solutions, a safe level of exposure for injectables was shown to be a small fraction of that 850 mcg. Safety limits were now set for neonates at 4-5 mcg per kilogram of body weight, limited to 25 mcg aluminum per day (by regulation 21 CFR 201.323).
All injectable drug products were subject to this new limit… but not vaccines. Vaccines inexplicably remained at the 850 mcg limit.
The package insert for the Recombivax HB (HepB) vaccine shows its formulation contains 0.5 mg (500 mcg) of aluminum, with residual formaldehyde:
RECOMBIVAX HB® Hepatitis B Vaccine (Recombinant)
Suspension for intramuscular injection
Initial U.S. Approval: 1983
All formulations contain approximately 0.5 mg of aluminum (provided as amorphous aluminum hydroxyphosphate sulfate, previously referred to as aluminum hydroxide) per mL of vaccine. In each formulation, hepatitis B surface antigen is adsorbed onto approximately 0.5 mg of aluminum (provided as amorphous aluminum hydroxyphosphate sulfate) per mL of vaccine. The vaccine contains <15 mcg/mL residual formaldehyde.
The other HepB vaccine available for infants, Engerix, contains 250 mcg of aluminum. These vaccines are injected at birth, usually on day one, then again at 2 months and 6 months.
Manufacturer label information shows similar aluminum content in other childhood vaccines:
DTaP – 330-625 mcg. Administered at 2 months, 4 months, 6 months, 18 months, and 4 years.
HiB – 225 mcg. Administered at 2 months, 4 months, 6 months, and 12 months.
HPV – 500 mcg. Administered at 9 years, 10 years, 11 years.
Current vaccination schedules in which multiple shots are administered in a single visit exceed even the 850 mcg limit. For parents following the CDC schedule, aluminum injected at the 2-, 4-, and 6-month “Well Baby Visits” can exceed 1000 mcg. The CDC has NEVER safety tested this cumulative load received in multiple shots. Physicians for Informed Consent show aluminum content for the childhood vaccines:
Why does the 25 mcg limit apply for other injectables but not vaccines?
The mid-1900s study that determined the 850 mcg limit may present the answer to that question. The purpose of that study was not to determine safety — it was to find out the amount of aluminum needed to provoke an immune response. A 1947 document related to the manufacture of diphtheria toxoid states, “In all instances, the amount of aluminum used shall be the minimum needed to accomplish the purpose intended.”
In “Reconsideration of the immunotherapeutic pediatric safe dose levels of aluminum,” James Lyons-Weiler and Robert Ricketson note (my emphasis):
“FDA regulations require safety testing of constituent ingredients in drugs (21 CFR 610.15). With the exception of extraneous proteins, no component safety testing is required for vaccines or vaccine schedules. The dosing of aluminum in vaccines is based on the production of antibody titers, not safety science.”
If an adjuvant does not create an inflammatory response and antibodies are not produced, the vaccine essentially does not work at all. Given that aluminum in vaccines is in the hundreds of micrograms, it would appear that at levels which might be considered safe — 25 mcg or less — the adjuvant is unable to stimulate the production of antibodies.
And if antibodies are not produced, a vaccine cannot provide any protection against the disease targeted by the vaccine. It will not “accomplish the purpose intended.”
Therefore, the allowable dose “was based on immunological considerations — not on data demonstrating this amount to be non-toxic when injected into children. The limit was never intended to indicate an amount of aluminum that could be considered harmless to children.”
At the 4-5 mcg per kilogram of body weight or total 25 mcg per day limit applied in 1997 to other injectables, the aluminum load in even one shot should not be permissible. In The Vaccine-Friendly Plan, pediatrician Paul Thomas discusses the 250 mcg dose of aluminum in a single HepB shot:
“If your baby weighs 7 pounds at birth (approximately 3 kilograms), the FDA stipulations suggest that the maximum safe dose for that newborn is 15 micrograms, sixteen times less than what is given in one hepatitis B vaccine. Since infants may not be able to effectively rid their bodies of aluminum, the truth is that no amount of aluminum is safe. By giving infants this shot, according to the FDA’s own calculations, we are literally poisoning them.”
————————————
[2] MERCURY
The type of mercury in vaccines – ethylmercury – is NOT harmful to us. It prevents microbial growth in multi-dose vaccines.
No childhood vaccines contain mercury.
THE FACTS / MERCURY:
“[Thimerosal] is toxic… Mutagenic in mammalian cells.“
May cause “decreased offspring survival, and offspring nervous system effects including mild to severe mental retardation and motor coordination impairment.”
—from the manufacturer’s Material Safety Data Sheet
“Comparing toxicity in two forms of mercury is like comparing the benefits of being shot with a .38 caliber bullet rather than a .45 caliber bullet. Most people would prefer Door #3: no bullet at all.”
—Gavin de Becker,
“Forbidden Facts: Government Deceit & Suppression About Brain Damage from Childhood Vaccines”
Entire books have debunked the absurd statement “ethylmercury is NOT harmful to us.”
Mercury is the third most toxic element on earth, 500 times more poisonous than lead. Thimerosal is the trade name for the 50% ethylmercury solution used since the 1930s as a preservative in vaccines. Contrary to our health department’s claim, it is highly neurotoxic — dangerous enough to cause “decreased offspring survival” as Eli Lilly was required by law to disclose in its Material Safety Data Sheet for thimerosal.
New works have expanded on Robert F. Kennedy, Jr’s 2015 book on thimerosal mentioned earlier, not least the unexpected perspective of internationally recognized criminologist Gavin de Becker, quoted above. More than a review of the scientific literature, his best-seller Forbidden Facts: Government Deceit & Suppression About Brain Damage from Childhood Vaccines, documents how government, industry and academia routinely conspired to create a false narrative and deceive the public.
De Becker begins his chapter on mercury with this definition:
“A silvery white poisonous metallic element used in batteries and in the preparation of chemical pesticides.”
He continues,
“…and in vaccines given to children and pregnant women.”
Injected ethylmercury has been shown to deposit in the brain and other organs far more readily than the much-publicized methylmercury in fish, which pregnant women are warned to avoid.
A 2005 University of Washington study funded by National Institutes of Health compared brain mercury levels from injected ethylmercury (thimerosal) to equal amounts of orally ingested methylmercury. The study demonstrated that while ingested methylmercury generally remains in the bloodstream, injected thimerosal crosses the placenta and blood brain barriers at high levels. This is the exact mechanism Miller described in the SIDS report above, and shown in the illustration regarding aluminum.
Once deposited in the brain, thimerosal converts to inorganic mercury and remains trapped there, resulting in neuroinflammation. Autism and other neurological disorders are associated with this accumulated mercury in the brain.
Our health department tells us that thimerosal “is NOT harmful to us,” while also assuring us that it’s not in childhood vaccines. If it is so harmless, why would it have been removed from them?
That brings us to the seminal study about a possible link between thimerosal and autism mentioned earlier. In 1999 the CDC commissioned epidemiologist Dr. Thomas Verstraeten to do a study to put to rest concerns about thimerosal causing autism. The findings were so alarming—infants exposed to high levels of thimerosal during their first month of life had 7.6 times higher risk of autism diagnosis than their unexposed peers—that a secret emergency meeting was convened.
To avoid public scrutiny the June 2000 emergency meeting was not held at the CDC headquarters in Atlanta, but instead at the Simpsonwood Retreat Center in Norcross, Georgia. CDC and other government officials, university experts and pharma reps spent two days discussing the problems raised by this study and strategizing how they would hide the results from the public.
“The number of dose related relationships [between mercury and autism] are linear and statistically significant,” said Dr. William Weil from the American Academy of Pediatrics. “You can play with this all you want. They are linear. They are statistically significant.”
The attendees were then asked What should we do now?
The group identified as consultants “were unanimous in saying that additional research was needed.” An immunologist told the assembled participants that he’d just taken an emergency call in which he’d advised his daughter-in-law who had delivered his first grandchild not to accept any mercury-laced vaccines. Given the risk, his family was not going to get any of those shots.
At the end of day two, Dr. John Clements from the WHO’s Expanded Program on Immunization summed up the elephant in the room — any information leaking to the public that could lead to vaccine hesitancy was not permissible:
“My mandate as I sit here in this group is to make sure at the end of the day that 100,000,000 are immunized with DTP, Hepatitis B and if possible Hib, this year, next year and for many years to come, and that will have to be with Thimerosal containing vaccines unless a miracle occurs and an alternative is found quickly and is tried and found to be safe. So I leave you with the challenge that I am very concerned that this has gotten this far, and that having got this far, how you present in a concerted voice the information to the ACIP in a way they will be able to handle it and not get exposed to the traps which are out there in public relations.”
Given the “sensitivity of information,” sharing information outside that room was “embargoed”. Every page of the study was stamped “DO NOT COPY OR RELEASE” and “CONFIDENTIAL”. The full transcript of the Simpsonwood meeting was later obtained through a FOIA request.
Findings from the original Verstraeten Study shown above — “Increased Risk of Developmental Neurological Impairment after High Exposure to Thimerosal-Containing Vaccines in the First Month of Life” — never saw the light of day. Instead the CDC “massaged” the data and in 2003 released a reworked, fraudulent version of the study loudly trumpeting that thimerosal did not cause autism and other neurodevelomental problems. It’s the same playbook that CDC whistleblower William Thompson exposed decades later regarding the CDC’s study of the MMR vaccine and autism.
De Becker notes that the CDC, FDA and vaccine-makers came up with a “magnificently creative idea” to explain away “that ethylmercury was somehow not toxic”:
“They began to float a new idea: that ethylmercury is way different from other forms of mercury. Sure, it’s mercury — but it’s the gentle, benign, happy-baby mercury that’s not worth worrying about.”
The CDC’s cover-up of thimerosal’s toxicity included statements like:
“Thimerosal contains ethylmercury, which is cleared from the human body more quickly than methylmercury, and is therefore less likely to cause any harm.”
“The human body eliminates thimerosal easily. Thimerosal does not stay in the body a long time so it does not build up and reach harmful levels.”
Thimerosal has never been demonstrated to clear the body. As in the 2005 study mentioned above, as well as a more recent 2012 study by Croatian researchers, when thimerosal is injected it clears the bloodstream quicker than the ingested methylmercury in fish because rather than being filtered and excreted, the tiny ethylmercury molecules travel to vital organs and the brain. And while most of ingested methylmercury is excreted in a matter of weeks, injected ethylmercury in thimerosal metabolizes to the deadliest form of mercury known, inorganic mercury, and remains in the brain and organs for decades. As with lead poisoning, mercury loads are cumulative. [more info]
While the CDC refused to admit publicly that thimerosal in shots is neurotoxic, the US Public Health Service and American Academy of Pediatrics did call for the immediate removal of thimerosal from infant vaccines.
The CDC’s mantra “Mercury in Vaccines does NOT Cause Autism” persisted on their website and in other information they disseminated… at the same time announcing that mercury would be removed from childhood vaccines. Vaccine manufacturers were told to quietly phase out thimerosal from the childhood schedule, but stocks of existing thimerosal-preserved vaccines continued to be administered over a two-year period until they were used up.
As in the HepB vaccine mentioned previously, the new and improved thimerosal-free formulations typically substituted toxic aluminum for the toxic mercury.
While no longer in most infant vaccines, thimerosal has NOT vanished from the childhood schedule as claimed. It is still used in some flu shots and other vaccines. So in addition to fetal exposure in utero from flu and other shots given to pregnant mothers, children following the CDC’s vaccination schedule play the mercury lottery twenty times, getting their flu shots at 6 months, 7 months, one year, then annually every year until they’re 18.
RFK Jr’s 2015 compilation of hundreds of peer-reviewed studies erases any doubt that thimerosal is a potent neurotoxin that causes neurological damage, from tics to autism. In de Becker’s more recent research of the scientific literature, newer studies continue to show that exposure to ethylmercury can cause neurological injury, developmental problems, impaired language skills, and autism. The last review he cites is a meta-analysis:
“This review found 91 studies that examine the potential relationship between mercury and ASD autism from 1999 to February 2016. Of these studies, the vast majority (74%) suggest that mercury is a risk factor for ASD [Autism Spectrum Disorder], revealing both direct and indirect effects. The preponderance of the evidence indicates that mercury exposure is causal and/or contributory in ASD.”
He further notes that studies that denied a risk were nearly always generated by the groups promoting vaccination, rarely by independent researchers.
The claim by health agencies that injected ethylmercury is benign becomes even more inconceivable in light of the fact that the EPA classifies the thimerosal in vaccines as toxic hazardous waste. The limit for mercury in drinking water is set at 200 parts per billion per the EPA’s Toxicity Characteristic Leaching Procedure (TCLP). The mercury in multi-dose flu shots preserved with thimerosal, injected directly into the body, is 250 times higher—50,000 parts per billion.
Thimerosal as a Vaccine Preservative, a summary prepared in 2025 for the CDC’s Advisory Committee for Immunization Practices (ACIP), notes that “thimerosal-containing vaccines exceed the TCLP threshold by orders of magnitude and are classified as D009 Hazardous Waste.”
PharmEcology’s Disposal Guidelines for the 2025-2026 Flu Season spells out:
“[A]ny vaccine waste containing thimerosal as a preservative should be managed as a toxic hazardous waste. As a result, all full or partially used multi-dose vials of the seasonal flu vaccine should be disposed of as federally hazardous waste, waste code D009 for mercury.”
Shocking as it sounds, had the mercury-laden childhood vaccines that were phased out from 2000 to 2002 not been injected into babies and children, pharma would have been required to dispose of them as hazardous waste. But Jefferson County Public Health tells us that injecting that same thimerosal into developing infants is perfectly safe.
In the UK, Denmark, Austria, Japan, Russia, and all Scandinavian countries, vaccine makers are not permitted to use thimerosal in any childhood vaccines, including flu shots.
Criminologist De Becker observes that if the CDC’s patently false statements about thimerosal—the same ones made by our health department—were given under oath, the claimants would be accused of perjury.
————————————
Sadly, aluminum and mercury are not the only toxic substances in vaccines. Among other dangerous additives that should “make folks nervous” are:
Polysorbate 80. A surfactant (emulsifier) that enables other substances in vaccines like aluminum and mercury to cross the blood-brain barrier. It is linked to infertility, known to cause cancer, and banned from injectables in most of Europe.
Phenol/2-Phenoxyethanol. A germicide and potential allergen, used as a preservative. Neurotoxic and may cause lung and liver irritation, hormone disruption, and kidney and nerve damage;
Formaldehyde. Another preservative. Commonly used to embalm bodies, it is classified by both the National Toxicology Program and the International Agency for Research on Cancer as a known human carcinogen. It also oxidizes into formic acid, a neurotoxin which can damage both the liver and the kidneys.
Our vaccine study group’s 2017 guide provides an overview of the many ingredients disclosed in package inserts as well as undisclosed contaminants found in childhood shots:
The DTaP vaccine provides a good example of the toxic soup typically injected in just one shot.
From the 16-page package insert of Infanrix, a DTaP vaccine “indicated for active immunization against diphtheria, tetanus, and pertussis as a 5-dose series in infants and children aged 6 weeks through 6 years”:
Along with other chemicals, DTaP formulations contain aluminum, formaldehyde and polysorbate 80. The polysorbate 80 helps deliver the aluminum into the brain and other organs; the formaldehyde has the potential to damage the liver and kidneys, as well as cause cancer. Depending on the manufacturer, the DTaP shot may also include bovine extract, monkey kidney tissue (suspected to contain SV-40, a cancer-causing virus), and neomycin sulfate or polymyxin B, both antibiotics.
At the core of the vaccine narrative, the notion that a vaccine only contains a small amount of virus, bacteria or other antigen in a neutral solution to mimic natural disease is a fairy tale. In any product except vaccines, injecting toxic metals and chemicals into children and most especially pregnant women and developing babies — at levels far beyond safe limits established by regulatory agencies — would be considered criminal.
———————————————
Part 2 will discuss the remaining claims in our health department’s ad. Are there “no credible studies that link vaccination to chronic disease”? Is it true that “vaccines are tested more than any other medicine you could give your kid”?
We will also share Jefferson County Public Health’s response to questions we sent them about the ad, including a request for sources/evidence to support their claims.
Finally, we’ll take a look at the rise in vaccine hesitancy that may have provoked JCPH’s creation of this ad, and at challenges being made to the CDC’s current childhood vaccine schedule. Efforts to rein in pharma’s capture of health agencies, medical groups and the vaccine narrative are causing a pitched battle, and the institutions entrenched in the religion of vaccines are doubling down to maintain their control.
by Annette Huenke and Ana Wolpin | Oct 14, 2025 | General
When Jefferson County PUD customer-owners who opted out of “communicating” smart meters were notified between September 6th and 12th that their $5 monthly opt-out fee was proposed to triple, more than 70 letters responded to a request for feedback.
Most letter writers raised objections to the proposed hike, with concerns voiced that not enough time was given for feedback — asking for a delay on the decision slated for the meeting just days later on Sept. 16. Some questioned the validity of the fees proposed based on consultant FCS’s report. Many suggested that a simple self-read option be made available as described in our Sept. 10 article, PUD to Triple Monthly Smart Meter Opt-Out Fee?
This article will examine:
- the Sept. 16 PUD meeting and decisions,
- the inflated costs attributed to opt-out customers for manual meter reads,
- the focus on opt-out customers in the larger context of the PUD’s overall outlays,
- cost recovery inequities, and
- the industry agenda to create a punitive climate to discourage opt-outs and force all electric customers into the smart grid.
Recap of the September 16th Meeting
It was announced at the outset of the Sept. 16 meeting that staff had come with an alternative resolution to the one initially proposed. The new proposal still called for the immediate implementation of every-other-month reads, done by meter readers on even-numbered months, with usage charges estimated on odd-numbered months.
However the implementation of the $15 opt-out fee increase would be postponed until July 2026. Staff continued to recommend that the low-income discount no longer apply to the opt-out fee.
Eight opt-out supporters showed up to the meeting, with an additional dozen or so appearing on the Zoom platform, some wishing to voice their opinions. Between that modest in-person showing and those on Zoom, commission chair Jeff Randall decided to reduce the time for public comments from three minutes to two, even though it was unclear how many of that total would want to speak.
Most commenters mentioned the desire to assist the PUD in lowering costs by reading their own meter, as is available with the Snohomish PUD. After the comment period closed, General Manager Joe Wilson explained the genesis of Snohomish PUD’s self-read program (at 105 min.).
The reasons given for why we will not be going down the SnoPud “take a photo of your meter” path was as follows, in GM Wilson’s words:
“[At] Jefferson PUD, we’re very stretched financially, and we’re using off-the-shelf utility software. We don’t customize it, we’re trying to be economical in our software expenses. So while I understand that it was being perceived in the community to be very straight-forward, staff at Jefferson PUD don’t see a clear path to be able to feasibly do this economically. We believe that there’d be software development charges, union negotiations because this would transfer from a particular union representing the meter readers to a different union, may transfer to a different union processing internally or we’d still have to have the meter readers sit in a terminal. So we have to be respectful to our unions where this work is potentially bridging a gap, and develop new processes to make this happen. At a high level, it doesn’t seem economic to try to do that work, and frankly, then we, following these same cost of service principles, expect the folks that are requesting the service to cover those costs. I see a very high probability that those costs would be higher than the costs of this [current proposal].”
SnoPud has roughly 18 times the customer base of JPUD, which confers a great deal more resources, many more employees and a much larger budget. Wilson pointed out that this affords them the luxury of “specialized products like this” (customized software to accept photographic reads).
Little did we know, the notion of self-reads of any sort was Dead On Arrival.
Regarding staff’s stated plan to allow two weeks for feedback and incorporation of that input into subsequent resolutions not being honored, GM Wilson offered “apologies for if I misspoke.”
Staff was tasked by the commission to bring the finalized resolution to the regular meeting on October 21st, with Commissioners Jeff Randall and Dan Toepper expressing their sustained reservations about the $15 fee.
GM Wilson recommended comments be sent to the commissioners and staff by October 15th for consideration of incorporation into the new resolution. You can write your commissioners at any time to express your concerns.
What Does a Manual Read Actually Cost?
Consultant FCS asserted that it costs the PUD $28.30 to provide on-site meter reads. Staff’s proposal to raise the current $5 charge to $15 is based on reducing those on-site reads by half to every other month.
But that $28 figure is inflated. Regional corporate utilities price their manual reads from $7.50 to $10, as we will see below.
Let’s look at FCS’s cost breakdown of the $28.30.
We’ll discuss just two of these categories here.
$16.37 Meter Reading:
When the opt-out policy was adopted in 2019, the PUD was paying meter company Landis+Gyr somewhere in the $4.50-$4.80 range for their meter readers to manually read some hundreds of our meters every month. If it is now costing in excess of $16 for a PUD meter reader to do the same, there are clearly efficiency issues that have not been addressed.
According to former GM Kevin Streett, every opt-out read requires an individual service order to be generated every month. From the discussion at the PUD’s Aug. 5 special meeting it also appears the reads are mixed in with other business in the field.
Why is there not a schedule and program designed to maximize efficiency? The same question applies to the customer service charge. Why no automated system?
$8.91 A & G Overhead:
Commissioner Randall noted at the August 5 special meeting that administrative overhead such as “the commissioners spending time discussing this topic” (an example the consultant used to justify this charge) is already built into electric customers’ base rate. The recent hike in that base rate, now set at $33.50 for residential customers, covers meeting time and all other administrative costs. And, as we will see below, it also subsidizes other non-electric services within the PUD.
Charging opt-out customers a second time for administrative overhead when we are already paying for that in our base rate is “double dipping,” Randall rightly contended. FCS arguing to charge us twice for this demonstrates an agenda that we will speak to later.
Opt-Out Customers Singled Out for Scrutiny
At the Sept. 16 meeting, co-author Annette Huenke commented on the PUD’s outsized focus on the relatively piddly cost of the opt-out program compared to the multi-million-dollar broadband project. She challenged the PUD to run the same fine-toothed comb through that service category’s figures and ask the broadband customers to cover all the costs the electric customers have borne for them for the last five years — including the time commissioners have spent at broadband meetings.
GM Wilson highlighted that comment, saying that “cost recovery in our service lines is an area of passion for me, too.” He continued, “the reason we’re not doing that well in broadband is that the community sees an opportunity to capture a lot of grant money, but I agree with you that we need to get back to cost recovery in our service lines.”
One doesn’t hear the same sense of urgency for correcting that situation, though the cost to the PUD and the customer-owners is orders of magnitude greater.
What about those “smart” meters that are currently requiring manual reads?
When the Smart Meter Objectors’ Group (SMOG) first got involved at the PUD, the utility had enlisted meter manufacturer Itron to begin replacing the malfunctioning meters within the leftover PSE inventory. Itron was also a front-runner for winning the contract for upgrading our system to smart meters.
Our digging revealed that a Radio Frequency Propagation Study (Rf Prop Study) had been requisitioned some years earlier. These studies are critical to understanding how terrain could impact frequency transmissions from distances promised by industry. Iowa and Nebraska — where the landscape is flat as far as the eye (or radio frequency) can see — is one thing; the Pacific Northwest and specifically Jefferson County is another.
We’d already heard of the tens of thousands of meters that were failing to communicate with receivers in the massive rollout in British Columbia, where the terrain is very similar to western Washington. Radio frequencies are hampered by moisture, foliage and elevation changes. Over greater distances, structures can be problematic, too.
Itron conducted its Rf Prop Study using satellite data, rather than an on-site visit, in 2014. A records request revealed that, on July 2, 2014, JPUD’s contracted representative, Byron Howells, wrote to Itron’s rep, inquiring about that matter:
Rob —
Did the Rf Prop Study Report show up today?
Itron’s rep, Rob Rickard, responds:
Prop completed but it does not look good for FN [frequency network] — I’ll call you later when I’m driving.
Half an hour later, Byron Howells replies:
No it does not look promising.
Based on what I am seeing with the MCLite, the count is about 150 more collection/repeater points than I thought we would require.
Using the study numbers we would need a CCU for every 100 Meters. In the sparsely populated South that ratio could drop below 50:1.
Any chance of a Pilot to see what the RF Prop is really like?
The rest of the discussion was off the record, in a phone call. Though this contains a lot of industry jargon, our research at the time showed that the collectors were quite expensive. This may help explain why this system that serves roughly 21,000 customers cost $5 million.
What we learn from this is that our PUD knew more than a decade ago that, at best, there would be holes in their mesh network, and a significant number of meters would have difficulty communicating with radio receivers assigned to them. Thus the meters would have to be read manually.
Why don’t we have consultant FCS run their fine-tooth comb over those manual reads and give us an estimate of what they are costing the utility each month? As reported in our Sept. 10 article, a records request from August 14th showed 310 meters “offline” at that particular moment in time, ie. not communicating with the PUD. That’s 60% of the opt-out meter customers! Surely they also require a service order to initiate the truck rolls. What happens if the meter transmission is simply not capable of reaching the collectors?
Opt-out customers are basically being told they will have to subsidize the smart meters that can’t function as designed, as well as those that do. It should be noted here that the commissioners have asked staff what the cost savings amount to from the smart meter rollout, and are told that this number is not known.
Cost Recovery Across Service Divisions is a Pipe Dream
A brief discussion ensued at the Oct. 6, 2025 budget hearing regarding the fiscal status of the PUD’s water and broadband divisions. There are roughly 5,000 water customers (versus ~21,000 electric customers) and the department runs a chronic deficit. The electric side, primarily through the base rate, is fully subsidizing the water side.
Fewer than half of county residents needed the PUD’s broadband program, as they were already being served by various carriers. The broadband division is also running a deficit. The electric side is subsidizing broadband, too.
It gets worse.
The percentage of property taxes Jefferson County allocates to the PUD (.75) amounted to $605,702 for 2025 (assessed in 2024). A full 80% of that is going to broadband; 20% goes to the water department. Exactly zero of the property taxes we pay go to offset the base rate for electric customers.
GM Wilson noted that “opt-out [meter] readers are not doing a task that benefits all electric customers.” Neither are broadband technicians and water meter readers. And technicians that attend to malfunctioning “smart” meters are not doing a task that benefits those who chose not to have a transmitting meter.
When we raise the issue of the unfairness of opt-out customer-owners having to help foot the bill for a system they don’t benefit from in addition to the one they do, commissioners nod in agreement and say “you’ve got a point.” When the commissioners raise the issue of the electric side subsidizing the other services, staff nods, makes modest excuses and goes back to work. That’s just the way it is, fellas.
The playing field cannot be leveled. So let’s stop the pretense that parity is possible, and accept the existing inequalities — across the board.
The Planned Phase-out of Analogs Continues Apace
The PUD has now halved the cost to the utility for opt-out reads by reading meters every other month. At the last several meetings, GM Wilson has made it abundantly clear that he intends to phase out the electro-mechanical (analog) meters before long. The reason drifts from there not being spare parts, or that we won’t be refurbishing “obsolete” meters (though the near-new malfunctioning digital meters are regularly refurbished), to the need for all the meters to be the same. However, at the Sept. 16 meeting, one of the commissioner questions that Wilson read aloud asked if there was a charge for installing an electro-mechanical meter. He said that was not an option, and that “the PUD has an inventory of Itron non-communicating meters that would get deployed.”
Those non-communicating meters are digital one-way transmitting meters, the same type that the PUD was using prior to the smart meter rollout. So the meters won’t all be the same after all — until they insist that we submit to having smart meters installed with the outgoing transmitter turned off.
They will still need to be read manually (just like all the smart meters around the county that don’t work properly now), but the incoming transmitter will not be turned off. What you do in your home will not be secure from surveillance, and voltage transients (dirty electricity) will be transferred throughout the home’s wiring by the meter’s power supply (SMPS).
The Industry Agenda Behind the Singular Opt-Out Scrutiny
The FCS consultant emphasized the four utilities on their comparison slide showing $25 opt-out fees (bars at right) as a way to justify their inflated $28.30 figure (far right) at Jefferson PUD.
We know that’s what many utilities typically charge, but that those $25 fees are not based on costs. It is a nationwide strategy to discourage—and eventually eliminate—opt-outs by an industry that does not want holes in its smart grid.
In our prior process, when JPUD initiated an opt-out survey of all Washington state PUDs, one utility even said it out loud — they added a written note that they’d set their punitive fee “to discourage opt-outs.” And it worked. Very few customers had opted out.
One need only look at true costs for manual meter reads identified by for-profit corporate utilities PSE (Puget Sound Electric) and PG&E (Pacific Gas & Electric) to see the game. PSE and PG&E charge initial one-time fees (see chart above), but ongoing monthly charges are modest. PSE’s monthly read fee is $7.50; PG&E’s is $10. Those costs are all-inclusive — meter reading, customer service, overhead and taxes.
At Jefferson PUD, opt-outs are the only group of customer-owners accused of not paying their fair share. The much larger subsets of water and broadband customers, both subsidized by electric customers, do not receive equivalent treatment. Inflated calculations for opt-out customers are contrived to relieve a supposed burden on the larger customer base — costs which are minuscule in the context of the utility’s spending. That is in keeping with the industry narrative to drive opt-outs from the mix.
The PUD’s announcement proposing to triple the current $5 charge had the desired effect. Quite a few customers responding to the request for feedback said they couldn’t afford the increase and would be forced to accept a smart meter instead.
Given the volume of inequities within the system, those who choose to opt-out need to stand firm that we should not be the sole targets of the PUD’s sudden fiscal scrutiny.
Keep the fee at $5/month until the other, far costlier inequalities within the system are resolved. If this doesn’t happen, we can presume that the opt-out fee is indeed punitive, intended to drive everyone into the smart grid, despite our legitimate concerns around the “smart” meter technology.
by Ana Wolpin and Annette Huenke | Sep 10, 2025 | General
Allowing only days for customer-owner feedback, Jefferson County PUD is proposing a significant hike in fees for those who opted out of smart meters.
In a letter dated September 3, 2025, the PUD just informed customers with non-transmitting electric meters of an impending cost increase — tripling their current $5 per month opt-out fee to $15 per month. Low-income customers who previously had no monthly read fee would see an even greater increase, from zero cost to $15.
The letter invites customer feedback:
“I am reaching out today regarding upcoming changes to our communicating meter opt-out policy. You are receiving this letter because you have been identified as one of our customers who has chosen to opt-out of a communicating electric meter.”
“In an effort to maintain full transparency and receive feedback from community members impacted by possible upcoming changes, I am inviting you to provide feedback to the PUD regarding proposed changes…”
“We want to partner with you. If you have any suggestions or questions, please reach out to us at customerservice@jeffpud.org with the subject line of “Opt-Out Feedback” on or before September 12th, 2025. We will take this feedback into consideration.”
We received this letter on September 6th, leaving six days for feedback. One opt-out customer contacted us today, September 10th, saying they had just gotten the letter, leaving two days to respond. Interestingly enough, at the most recent regular meeting (@139 min. mark) on September 2nd, new General Manager Joe Wilson said we would be given two weeks to provide feedback.
The PUD’s “effort to maintain full transparency and receive feedback” hadn’t materialized as a news alert about the opt-out rate in any of the PUD’s monthly newsletters. Nor can we find this proposed fee increase/invitation for feedback on the PUD’s website. The only notice regarding these proposed changes has come in a last-minute letter offering less than a week for responses.
Why this extra cost?
Scientific evidence remains clear that transmitting (“communicating”) meters affect biological systems, not just in humans, but flora and fauna as well. For those of us opting to avoid the dangers of transmitting meters by choosing either a relatively benign non-communicating digital meter or an even safer analog meter, a meter reader comes to our homes to read electrical usage every month. The $5 fee was established to cover the cost of this monthly read. It was based on what it cost the PUD in 2020 when manual reads were contracted out and the opt-out policy was adopted.
The PUD’s letter informs us that according to a 2025 consultant’s report, the actual cost of the monthly read is now $28.30. The utility’s proposal is to reduce that cost to $15 by cutting the onsite visits in half, “sending technicians to manually read the meters every other month” instead of every month. Six readings a year rather than twelve.
The authors of this article are two of the founders of SMOG — Smart Meter Objectors Group. We worked from 2017 to 2020 to prevent a smart meter rollout in Jefferson County and develop an opt-out from transmitting meters.
Through these efforts, in late 2019 a pause was put on pursuing a smart meter program and in January 2020 the existing opt-out policy was adopted. When Covid lockdowns hit, community input was decimated. The PUD’s Citizen Advisory Board (CAB) was disbanded, in-person PUD meetings ceased, and direct communications with our commissioners was compromised. In the absence of community engagement, the utility resumed its smart meter efforts, starting a rollout in 2022.
Previous articles we’ve written about SMOG’s history, about the smart meter replacement program, and about the dangers of smart meters include Smart Meters Coming to a Neighborhood Near You! and Will a Smart Meter Harm Your Health?
Simple Solutions to Meter Reading Fees Already Exist
According to a recent Public Records Request, there are 486 PUD customer-owners currently opting out of transmitting meters. For many of these customers, this proposed fee hike is significant. Going from $60/year to $180/year, that’s another $120 increase on top of the general rate hikes that began this July. And for low income residents who have not had to pay any extra fees, it will create an even greater hardship, increasing their annual utility costs by $180.
From our research, this financial hit is easily avoidable.
Simple, low-cost alternatives to PUD employees reading meters onsite are already successfully employed by other utilities. These models do not require monthly or even every other month meter reader visits.
A Washington state PUD we spoke to when we first organized SMOG, which then had mostly analog meters, had its customers read their own meters every month — they are called self-reads. A customer could either call in or send their reading to the utility by a certain date. No technician was required onsite for 11 months. Once a year they sent a meter reader to make sure the customer was providing accurate readings. That PUD has since replaced all their analogs with transmitting meters and no longer uses that system.
But an even easier method is currently in use by Snohomish PUD. They began a smart meter rollout in 2023, and expect to complete the installation of 380,000 meters by the end of 2026. They offer two meter reading choices for opt-outs.
From Snohomish PUD’s website:
• Customer can have a PUD meter reader read their meter for a monthly fee of $25, or
• Customer can submit a picture of their meter and perform a self-read each month for a monthly processing fee of $5 per meter.
Snohomish PUD has 346,094 residential customers. It is the largest of the 28 PUDs in Washington state, the second largest publicly owned utility in the Pacific Northwest and the 12th largest in the nation. We spoke with one of the staff managing the opt-out program for clarification on their photo submission process.
In lieu of a meter reader coming to a customer’s property, the customer submits a photograph once a month showing their power usage through a convenient online portal at SnoPud’s website. Customers are given a 5-day window each month to make their submissions.
Simple. Easy. Snap a photo once a month, submit it electronically.
For Jefferson County PUD customer-owners, all that is needed is for our PUD to set up an online portal and/or provide an email address where we can submit the meter photo. A five-minute or less effort for the customer twelve times a year.
On the PUD’s end, no PUD meter reader is needed. No travel is required, no fuel is consumed, there are no complicated meter access issues.
That’s one consideration. But there is also an argument to be made that the current meter-reading program is more than fair — without increasing opt-out charges.
The True Cost of Opt-Outs Versus Smart Meters
Before Jefferson County’s smart meter rollout, we argued for a self-read option like the one described above as a NO-cost solution to minimize the need for monthly meter readers. Management felt that a $5 read fee was reasonable enough to bypass that approach. And low-income customers were given a break from that extra $5 charge.
The $5 figure was based on what the PUD was already contractually paying Landis+Gyr for reading a large portion of the meters that still had Puget Sound Electric transmitters on them. The cost they charged the PUD for reading each meter, many of which were failing, was actually slightly less than $5. While they were using a mechanical interrogation method for the transmitters still functioning, a significant number had to be physically read.
Now they claim we are not bearing the true cost of our choice to opt out. “Without these necessary changes,” the letter reads, “the option to opt-out of our communicating meters is not financially sustainable.”
But what ARE opt-out customers costing the utility versus smart meter customers? Are the opt-outs an unreasonable drag on the line?
To start, the $28.30 cost for monthly meter reads estimated by the consulting firm is debatable. On August 5th a special PUD meeting was held to discuss the opt-out policy (video here). The consultant presented their report and some discussion followed the presentation.
Of that $28.30, the expense for actually reading the meter — which the PUD paid less than $5 for in 2020 — is itemized as now costing $16.37. The remaining $12 includes items such as administrative overhead.
An example of administrative overhead given by the consultant at the August 5th presentation was the cost of “the commissioners spending time discussing this topic”! But these costs are already covered in our base rate, what one commissioner rightly described as “double dipping.”
Whatever the true cost, it doesn’t begin to compensate for the increased energy rates that opt-out customers are already bearing for a $5 million rollout of smart meters we don’t use or need. And beyond this massive outlay which has driven higher rates that we are ALL paying, we are also subsidizing extra costs from failure of the smart meter technology to live up to its hype.
Issues we warned about like meters failing to “communicate” likely create more demands on staffing than 486 non-transmitting meter reads once a month. On any given day, according to our recent Public Records Request (PRR), 300 or more smart meters may need attending to because they are “experiencing connectivity issues.”
As shown in this screenshot, on August 14 there were 310 smart meters offline (see blue bar, far right). Representing “a moment-in-time yesterday,” wrote the PUD Administrative Assistant who responded to the PRR, “310, this number fluctuates continually.” Sometimes it will be lower, sometimes it will be higher.
That figure is 64% of the total number of opt-outs! How much staff time is required to respond to hundreds of smart meters with connectivity issues that are not performing as needed? No such problem plagues our steady, reliable “non-communicating” analog and digital meters.
At the September 2nd regular meeting, staff gave a PowerPoint presentation that included this verbiage on a slide:
Continuing to allow Jefferson County Customers to offset the cost of customers choosing not to have a communicating meter goes against our desire to have customers generating the cost pay for the cost.
The opt-out fee is being treated as though it’s an anomalous inequity within the system. But is it? The fee is punitive, though not intentionally on the part of the PUD. It’s a misguided attempt to level a playing field that cannot be leveled.
• It is not fair that everyone is paying the same base rate that covers the cost of that $5 million smart meter rollout, when we who opt out aren’t using it.
• It’s not fair that when a few hundred of those meters regularly fail to communicate, those truck-rolls are considered the cost of doing business… but the truck-rolls for reading analog meters is considered a privileged gift.
• It is not fair that electric customers subsidized the build-out of broadband. How many hours (administrative overhead) did the commissioners spend in meetings discussing broadband? How will electric customers be reimbursed for that, applying the formula that was used to arrive at the opt-out cost?
• There’s unfairness in the higher cost of delivering services to all those spread-out homesteads in the south county.
These disparities cannot easily be remedied. That’s what the base rate is for.
Providing Feedback on Proposed Opt-Out Rates
The September 3rd unsigned letter quoted at the beginning of this article — “I am reaching out today” — appears to have come from staff, not from the PUD commissioners or the general manager whose names are at the top of the letterhead. It outlines the proposed rate hike discussed the day before at the September 2nd general meeting.
For those inclined toward number-crunching, here is the spreadsheet provided to the Commissioners by PUD consultant, FCS, to support their findings.
It was agreed at that meeting that a resolution on these proposed rates would soon be presented to the commissioners, possibly for a vote at their Tuesday, September 16th regular meeting, which takes place from 4pm-6pm. The meeting room is at the 310 Four Corners Road office building, to the right of reception.
We have learned through calls to the commissioners that feedback to them does not have to be received by September 12th, despite that deadline being given to respond to customer service. But it is critical that commissioners hear from opt-out customer-owners both AHEAD OF and AT the upcoming meeting. They plan to vote on this resolution at that meeting.
Email and phone contacts for our three PUD commissioners are:
Jeff Randall, District 1 – jrandall@jeffpud.org / 360-316-6694
Kenneth Collins, District 2 – kcollins@jeffpud.org / 360-316-1475
Dan Toepper, District 3 – dtoepper@jeffpud.org / 360-302-0448
You can cc emails to GM Joe Wilson at jwilson@jeffpud.org
Written feedback to the commissioners should be sent by Monday, September 15th to receive considered attention. At the meeting on Tuesday public comments are limited to three minutes. You can comment in person or via Zoom. More information about the meeting and about joining Zoom can be found here.
Addendum / Friday, September 12:
A Violation of Trust
At the PUD’s September 2 general meeting, when GM Joe Wilson said that a letter to opt-out customers would be going out with a two-week window for responses, he explained that after that two-week collection period, staff would go through a process of incorporating the feedback into a proposed resolution he would bring to the commissioners:
“After a two-week period hearing feedback, staff would attempt to incorporate that feedback into a proposal and bring it back to the board as a resolution for consideration.”
No such process took place. Not only was the stated two-week response time reduced to a matter of days, NO public feedback has been incorporated as part of the proposed rate changes.
Wilson did not even wait for the truncated Sept. 12 deadline to pass before putting the resolution that had been recommended on Sept. 2 in the Sept. 16 agenda packet. This morning, a full working day before the feedback deadline, the opt-out resolution was posted as an agenda item for Tuesday night’s meeting with the “Recommended Action” that the commissioners approve it as previously presented:
8.2 Opt-Out Presentation, Resolution & Calculations
Presenter: Joe Wilson, General Manager
Recommended Action: Make a motion to approve the Opt-Out Program Resolution as presented.
The resolution (p. 69) is exactly as discussed on Sept. 2 — no consideration or inclusion of customer feedback. The accompanying materials in the packet show the same staff recommendations made at that meeting where GM Wilson assured the commissioners a proposal would be drafted after gathering customer feedback and incorporating it. His actions demonstrate an effort to advance a predetermined outcome while his words professed otherwise.
How can the public believe staff was sincere in their letter requesting input and their stated desire to “partner” with us when our feedback has been ignored?
How can our new GM — completely disregarding a process he claimed would be followed — be trusted?
by Annette Huenke | Apr 4, 2025 | General
Amidst recent reporting, here and in the Leader, on the looming collision course of the city’s increasing expenses and diminishing revenues, news leaked recently to the Port Townsend Free Press indicates that our fearless leaders are nowhere near applying the brakes on runaway spending for consultants.
Later this month, City Hall and the library will be closed for four-and-a-half hours for a compulsory DEIB training. You may be as surprised as I was to learn of the fourth character tacked onto the end of the all-too-familiar Diversity, Equity and Inclusion label. That’s “B” for Belonging. More about all that later in this article.
Our streets are in deplorable condition — embarrassing, really. Our infrastructure is crumbling. For years, piles of our money have been thrown at “affordable housing,” none of which has yet to materialize, nor looks to be in the offing. With City Hall already limiting its days open to the public to Monday through Thursday, this required “training” not only means an additional loss of public hours, it is arguably another top-down driven, unnecessary and wasteful drain of city resources.
Who? What? When? And How Much?
The DEIB training will be conducted by Tacoma/Seattle-based Potential Unleashed Consulting on Wednesday, April 23rd. This won’t be their first appearance here. The city hired them for a 90-minute workshop in December last year, to begin city employees’ “learning journey.” Here is the HR memo to staff for the April event:
23 Apr 11 AM (4h 30m) Save the Date – City Training RSVP Hello all,
We are excited to continue our learning journey with Jahmad Canley from Potential Unleashed Consulting. Jahmad will facilitate an interactive workshop designed to help us continue our goal of building teams and cultures of belonging by:
• Examining the difference and linkage between invitation, inclusion and belonging • Learning practical frameworks to help us be more intentional about creating belonging in our environments
City Hall and the library will be closed on April 23rd to allow employees to attend this workshop. This workshop is considered part of your workday, unless your absence has been approved by your supervisor.
We look forward to your participation as it will offer knowledge and tools to support both [sic] your personal growth, your professional development, and our team’s overall success.
Thank you for your continued commitment to excellence.
According to their Linkedin account, Potential Unleashed Consulting was founded in 2010 and is headquartered in Seattle. The company has 11-50 employees and 5 “associated members,” one of which is their founder, Jahmad Canley. Articles and archives on their website do not date back further than 2020. This article referencing the Chamber of Commerce also notes the founder as Tacoma-based. Their 90-minute and 4.5 hour workshops offer this boilerplate syllabus:
DEIB Foundational Workshop
We will design and facilitate training to ground all participants in a set of shared frameworks, common language, and initial skills to understand how the work of DEIB functions in society and within organizations.
Participants will:
• Unpack and reflect on how race, gender, age, and other social identities set up all people to have different degrees of power and privilege in society.
• Examine key “both/and” concepts that support authentic relationships across social and hierarchical power differentials.
• Recognize the difference between blame and responsibility, and use that as a platform for accountable relationships.
• Differentiate between racism, prejudice, discrimination, and oppression, and explore how different forms of oppression intersect.
• Examine unconscious bias and its impacts of it [sic] on our culture.
• Begin to examine how bias functions within society and within organizations.
• Understand how our social identities give us different but equally significant roles in the work of DEIB, and how we can work together, strategically, to create justice and liberation.
• Begin to develop a “journey mindset,” the understanding that becoming an organization rooted in diversity, equity, inclusion, and accessibility is a process that requires sustained commitment to a vision.
The 90-minute workshop in December 2024 cost $3,800 for the ‘training,’ $748.28 for lunch, and however much 90 minutes times 130± employees’ salaries and benefits add up to. American Rescue Plan Act (ARPA) funds were used to cover the “training” cost then. The contract for the upcoming April event lists $7,300.00 for the vendor. Lunch will be provided by the city (taxpayers).
Then we have the cost of 4.5 hours of 133 employees learning about oppression that does not exist in their workplace, instead of doing the city’s business. A rough guess at salaries, benefits and full versus part-time indicates the tab likely to be in the $20,000-$30,000 range. (I welcome anyone to sharpen their pencils on that.)
A Long and Winding Road
Diversity training in the workplace was an outgrowth of JFK’s Executive Order (EO) 10925, signed on March 6, 1961.
President John F. Kennedy issues Executive Order 10925, which creates the Committee on Equal Employment Opportunity and mandates that projects financed with federal funds “take affirmative action” to ensure that hiring and employment practices are free of racial bias.
This order required education of federal employees to ensure they were in compliance with the new regulations. However, JFK felt compelled to spell out his intentions, lest they be misunderstood:
In a White House memorandum on the same day, he called for the elimination of any program that “(a) creates a quota; (b) creates preferences for unqualified individuals; (c) creates reverse discrimination; or (d) continues even after its equal opportunity purposes have been achieved.
Civil rights leaders meet with President John F. Kennedy in the oval office of the White House after the March on Washington, D.C. 1963. Library of Congress
The pressure on Lyndon Johnson to take it a step further during the ensuing tumultuous years was successful. Passage of the Civil Rights Act in 1964 went beyond JFK’s EO focus on federal funding proscriptions, expanding non-discrimination orders to restaurants, theaters, transportation and other public accommodations.
…it authorized the government to withhold federal funds from schools that had not desegregated in compliance with the 1954 Brown decision. In all, it contained 11 sections or titles. Title VI and Title VII are most important to the evolving connection between Civil Rights enforcement and affirmative action. Title VI covers discrimination in federally assisted programs, and Title VII covers employment discrimination in all large and medium-sized private businesses. [source]
What was often referred to as the “soft power of affirmative action” gradually morphed into exactly what JFK warned about in his memorandum, with the imposition of quotas in the early ’70’s under Richard Nixon.
Thus, affirmative action evolved from a vague concept buried in an executive order, to a set of legal regulations and practices. The shift from “weak” to “strong” methods of policy enforcement, it is important to recognize, was largely the result, not of legislative action, but of decisions made in the executive branch of the federal government and in federal regulatory agencies… toward the goal of achieving a color-blind society, and as a necessary means of ensuring that Whites would not discriminate against Blacks… [source]
Six decades later...
On June 29th, 2023, the U.S. Supreme Court — siding with Students for Fair Admission — determined that, at least as far as college admissions are concerned, we seem to have come full circle to the vision for potential outcomes noted in JFK’s 1961 memorandum. Chief Justice John Roberts delivered the majority opinion of the court:
Because Harvard’s and UNC’s admissions programs lack sufficiently focused and measurable objectives warranting the use of race, unavoidably employ race in a negative manner, involve racial stereotyping, and lack meaningful end points, those admissions programs cannot be reconciled with the guarantees of the Equal Protection Clause.
At the same time, nothing prohibits universities from considering an applicant’s discussion of how race affected the applicant’s life, so long as that discussion is concretely tied to a quality of character or unique ability that the particular applicant can contribute to the university.
Many universities have for too long wrongly concluded that the touchstone of an individual’s identity is not challenges bested, skills built, or lessons learned, but the color of their skin. This Nation’s constitutional history does not tolerate that choice.
Dissecting the Details of Woke Language in the Realm of DEIB
Diversity, equity, inclusion, belonging. We’re all familiar with the classic definitions of those common words. But do they mean what we think they mean when it comes to DEI?
D — It’s doubtful that anyone who lives in Port Townsend is opposed to seeing a broader representation of women and non-white people in government, or anywhere else. Gays and lesbians have been welcome here for decades. It’s unclear exactly when the “trans” activists hitched their wagon to legacy diversity, but this broadening of the definition is not seen as legitimate or welcome by much of the wider society. Immutable characteristics appear to matter to most people. Look no further than Rachel Dolezal, who lost her career and a lot more for pretending to be black.
E — There’s a critical distinction between equity and equality. Equality provides the same opportunity, rules and standards for all. Equity guarantees the same outcomes despite qualifications, effort and time invested. In this After Skool video, Equity, the Thief of Human Potential, economist and author Thomas Sowell explains how visions of “fairness” often go sideways…
If you want one or the other [equity or equality] you can go for it, but the one thing you cannot do is pursue both simultaneously. At least you cannot successfully do that.
I — The standard definition of “inclusion” is “to be included.” That’s not enough for DEI activists. Dr. Peter Boghossian explains: “‘Inclusion’… has the common meaning of ‘all people are welcome’. But it also has the woke meaning of ‘a space that restricts speech’. How can everyone feel included if speech is allowed that causes members to feel offended, and therefore excluded? Not everyone can, or so runs the woke logic. Therefore, to be truly inclusive, speech needs to be restricted.”
Further, “inclusion” to the DEI industry includes literal “exclusion” — good old-fashioned segregation — where whites have been denied participation and opportunities due to their skin color. Reverse discrimination is still discrimination. B — Belonging is a feeling. It cannot be measured. In the typical (of woke discourse) circular argument, belonging means one feels included. As I cast about the web for the logic of adding a synonym, of all things, to the alpha-string “DEI,” I came upon this:
Author Liz Fosslien differentiates the terms by describing diversity as “having a seat at the table,” inclusion as “having a voice at the table”, and belonging as “having that voice being heard.”
A nano-second ago, “having a voice at the table” meant that your voice would be heard.
The DEI Dilemma
According to the New York Times on March 13, 2025, “So far this year the number of companies in the S&P 500 that used the phrase “diversity, equity and inclusion” in annual reports has fallen by nearly 60 percent from 2024…” The DEI industry was recently estimated to be in the $8 billion range. Potential Unleashed’s two highest-profile clients, Microsoft and Amazon, are following the trend and backing away from their former commitments. In July, 2024, Microsoft cut the DEI cord:
In a surprising yet increasingly common move, Microsoft has quietly dismantled its team dedicated to diversity, equity, and inclusion (DEI). The decision, communicated via email to the affected employees on July 1, [2024] cited “changing business needs” as the reason for the layoffs.
On February 7, 2025, “Amazon’s annual report filed with the Securities and Exchange Commission for 2024 omitted a section included in the company’s prior annual report, which indicated Amazon has a focus on “inclusion and diversity” in hiring…”
The writing was on the wall before the 2024 election. This article from just a few weeks ago documents the pruning or shedding of DEI by 68 organizations with over 1,000 employees since 2023. In her book of that same year, The Adversity of Diversity, co-authored with Mike Towle, award-winning political scientist Dr. Carol Swain drops the responsibility squarely in proponents of the ideology’s lap: “… companies and corporations cutting their DEI programs are doing it because they know those programs and trainings are useless. All they really accomplish is to keep conflict going because that’s exactly what their job is…”
She continues “If heterosexuals and homosexuals, and Whites and Blacks and Hispanics, get along, there’s no need for a diversity officer…” 2023 looks to have been a watershed year for nudges away from the trend. Undoubtedly, the costly blunder by Anheuser-Busch of having wannabe-woman Dylan Mulvaney promote Bud Lite beer was a cultural turning point. Shortly afterward, the Biden administration’s macabre “Pride” celebration, which devolved into something that disgusted many Americans, compounded the insult by an order of magnitude.
…Rose Montoya (biological man living as a woman), who was one of the many people invited by the Biden administration, was recorded pulling down his dress and exposing himself while standing alongside two biological females living as men who were doing the same to show off their removed breasts.
Rose Montoya on the White House lawn, June 2023
The pendulum had swung too far. These misguided efforts at psychological manipulation have not gone down well with the vast majority of voters, many of whom turned out last November to say they’ve had enough of woke. The ascendancy of the aggrievement cult looks to be over.
A Cure in Search of a Disease
In the early 2000’s, my partner and I hired an African-American man to join our employees at the gallery we owned on Water Street. He also worked for April Fool and Penny, Too, and was universally loved by his co-workers and the community. He and I often spoke about racism, a matter I’d taken seriously from an early age. He never felt unwelcome in Port Townsend, he reported. He was just another one of ‘us.’ The city was so lily white, it was refreshing to see a brown face.
Our gallery represented Native American and Canadian artists who were more likely to be honored than looked down upon. Has something drastically changed in twenty years? Has a tide of bigotry and intolerance swept through and infected City Hall? Is there a cadre of city employees who staunchly refuse to use preferred pronouns? Unlikely. Dissatisfaction with the representation of women and people of color throughout the upper tiers of all of society was not new in the first decades of the 21st century.
The halls of congress itself have been a glaring example of the lack of diversity in our nation. The 2020 murder of George Floyd in Minneapolis set a ready torch to simmering frustrations coast to coast. The Black Lives Matter activist movement spawned by the 2013 acquittal of Trayvon Martin’s killer, George Zimmerman, had found its new raison d’être (and millions in shadowy funding). That summer of lockdowns, “social distancing,” and limits on gathering sizes for the majority of U.S. citizens saw dozens of city centers burned and looted by scores of rioters using Floyd’s murder as an excuse to incinerate — in many cases — their own communities.
While legacy media, and the Biden administration, largely defended these violent crowds as “mostly peaceful,” damage to hundreds of cities was estimated to be well over a billion dollars. Meanwhile congress, police and college officials were “taking the knee” to demonstrate their virtue, or fealty, to the perpetrators. Thus they were emboldened to press for more concessions.
Many of those cities have not recovered. Most of the vandals were not prosecuted. Very soon, the country saw cities allowing looters to gang-rob downtown stores, promising no prosecution if the valuables stolen amounted to less than $1,000. Those claiming victimhood who victimize are shown limited sympathy by the law-abiding. These felonious episodes contributed to the public perception that the fruit of Critical Race Theory (CRT) and DEI — woke, in other words — had begun to rot.
Port Townsend saw its own BLM actions in 2020, with a willing and apparently guilt-ridden “progressive” white populace in full support. The BLM organizers went looking for their racists, but struggled in vain to find them in this community.
Likewise, a hate-filled mob with a number of violent members was summoned by local gender activists to a “Let Women Speak” rally at the Pope Marine park in August of 2022 (see here, here, here, here, here, here and here).
Alas, despite the dishonest label applied by the city administration and legacy media, it wasn’t an “anti-trans protest.” It was a small group of females and their supporters standing up for the free speech and privacy rights of women and girls.
Where are the Metrics?
For many years, analysts have been attempting to qualify and quantify the benefits and risks of diversity training (DT). Does it actually further “justice and liberation,” an expressed goal of Potential Unleashed founder, Jahmad Canley? Last November, evolutionary biologist Colin Wright penned an article for Reality’s Last Stand titled “Why was this groundbreaking study on DEI silenced?” His question was directed at the New York Times and Bloomberg, two legacy media outlets who are generally known for toeing the establishment line. The research paper, Instructing Animosity: How DEI Pedagogy Produces the Hostile Attribution Bias, was published Nov. 13, 2024. Colin Wright distills it here:
Through carefully controlled experiments, the researchers demonstrated that exposure to anti-oppressive (i.e., anti-racist) rhetoric—common in many DEI initiatives—consistently amplified perceptions of bias where none existed. Participants were more likely to see prejudice in neutral scenarios and to support punitive actions against imagined offenders. These effects were not marginal; hostility and punitive tendencies increased by double-digit percentages across multiple measures. Perhaps most troubling, the study revealed a chilling convergence with authoritarian attitudes, suggesting that such training is fostering not empathy, but coercion and control.
The counter-narrative issues raised by this study were apparently too hot for the big papers’ presses to handle. Their refusal to cover this news is not an aberration. It’s how we got here. Another lengthy meta-analysis of available literature was published in the journal Annual Review of Psychology in 2022. The authors report:
In examining hundreds of articles on the topic, we discovered that the literature is amorphous and complex and does not allow us to reach decisive conclusions regarding best practices in diversity training. We note that scholars of diversity training, when testing the efficacy of their approaches, too often use proxy measures for success that are far removed from the types of consequential outcomes that reflect the purported goals of such trainings.
Taken as a whole, our review of the literature on DT reveals that, in light of the overarching goals of DT in these settings, the evidence regarding the efficacy of DT is for the most part wanting.
More importantly, perhaps, their review of the literature revealed a dearth of evidence that DT was solving an existing problem:
…measurements of systemic bias—such as minority representation, prevalence of workplace discrimination, and the promotion rates of historically marginalized employees—were largely absent.
As with the city’s training, the public is right to ask — why are we doing this now? Unless bias and bigotry are a frequently documented problem among city employees, taxpayers should not be funding this “journey.”
Dumbing Down is a Dumb Idea, Not a Solution
Racism and sexism have been a dehumanizing scourge around the planet for just about as long as we’ve been upright. These injustices won’t be remedied by more of the same, simply by trading places, censoring majority views, or shoving DEI struggle sessions down peoples’ throats. Counter-discrimination is backfiring badly, ultimately harming the very people it’s intended to help. Lowering academic standards has been a disaster.
There is growing pressure now to do away with SATs, GPAs and now even any shared conception of Standard English. What kind of world are we creating? In what way could this utter condescension possibly render a historically oppressed people suddenly equal? — Thomas Chatterton Williams [source]
The mean grade at Harvard and Yale, and many other elite schools, is A-; grade point average (GPA), 3.8. In 1960, the national GPA was 2.4.
Source: Report on Grading at Harvard College • By Elias J. Schisgall
We’re being told that objectivity, punctuality and math are racist (ironic, given that math was apparently birthed in Mesopotamia). Amorphous “feelings” are more legitimate than facts. Guess we can forget about mass transportation like buses and airplanes; they do run on schedules, after all. Should we be thinking twice about that next surgery? “Many have become weary of DEI in medicine, as deviations from merit-based practices can put patients in harm’s way.” The list of occupations that will endanger peoples’ safety if DEI continues to rule the day is long. Contemplate them for a while. Blogger el gato malo (no capital letters is his personal gimmick) states it succinctly:
any system that is not consciously and deliberately a meritocracy will become an anti-meritocracy.
this is not up for debate. it’s just emergent fact. as soon as you put people in charge of anything for reasons other than “they are good at it” and make the desired outcome of a system anything other than “competence and achievement” you get a system that will focus on creating failure.
vitally, teaching needs to resume moving at very different levels. you cannot teach the best and brightest in a curriculum and pace that the 30th percentile can keep up with. you need to let them run hard and learn fast. it’s the core intellectual capital of america and stifling these students out of some misbegotten fantasy about “equity” is grossly unfair to them. this is why experimentation and leveling and standards based acceptances are so vital here and why DEI has so badly damaged once elite schools. you cannot run them for dimwits without sacrificing the bright lights.
Speaking of lights, there is one at the end of this tunnel — and no, it’s not a train. The North Carolina Community College System (NCCCS) is linking with City University of New York (CUNY) and willing students of North Carolina to kick off a promising program called Boost, which “stands out as an appropriate post-DEI measure that focuses on economic need rather than race…”
The model has a history of success elsewhere, demonstrating notable increases in post-grad earnings, sustained full-time enrollment and completed 4-year bachelor degrees. “Based on a program developed by City University of New York and promoted nationwide by Arnold Ventures, the NC Community Colleges Boost model is recognized as the gold standard in accelerated workforce development in higher education.” You can read more about that here.
——————————
What exactly is the problem that city administrators aim to address with costly DEIB training for all employees of the City of Port Townsend? Was it certain behavior that precipitated it? Is it simply virtue-signaling to their base? Perhaps the unquenchable social-engineering thirst of the devotees that inhabit that building during work hours?
I wonder how the employees feel about having to attend these sessions. By focusing them on a “journey mindset” to “create justice and liberation,” will the public be better served? Do P.T. residents believe DEI “training” to be a wise use of their tax dollars, considering all the rest of what needs fixing here? It’s time for the city to get back to basics — doing the peoples’ business — FIVE days a week!

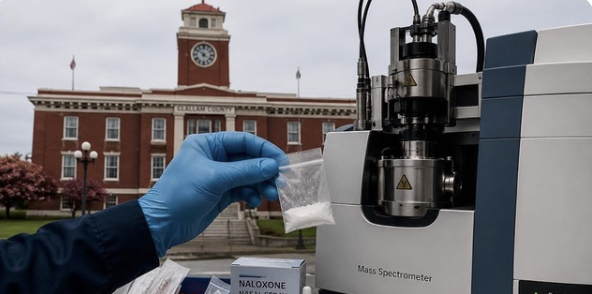



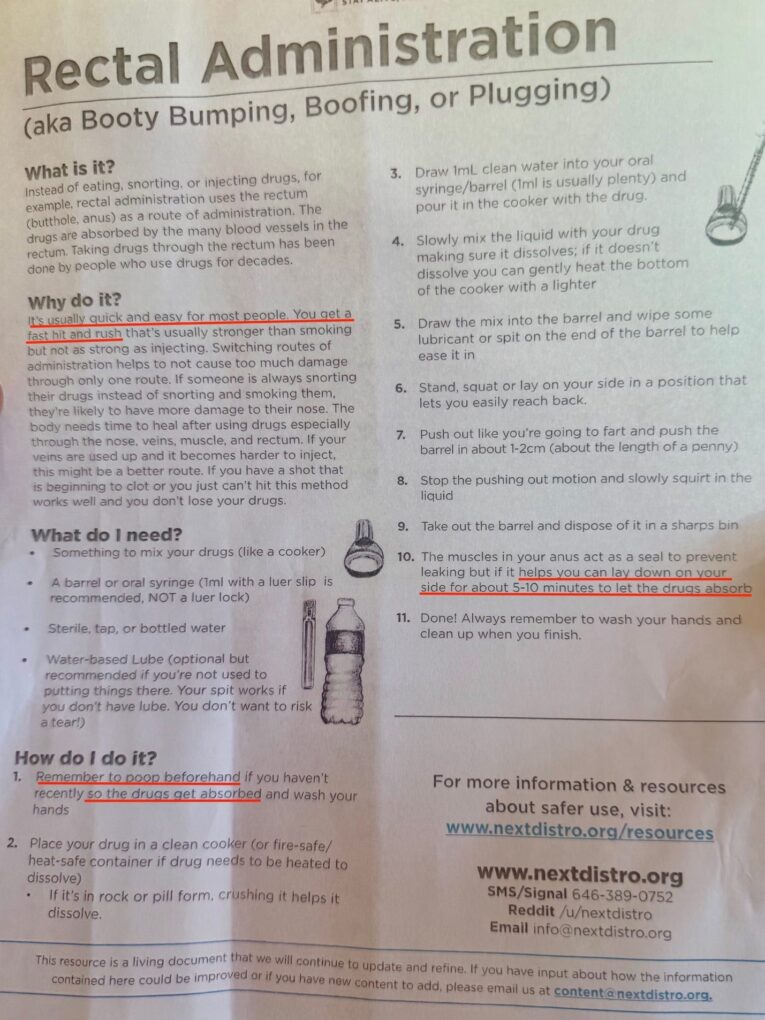
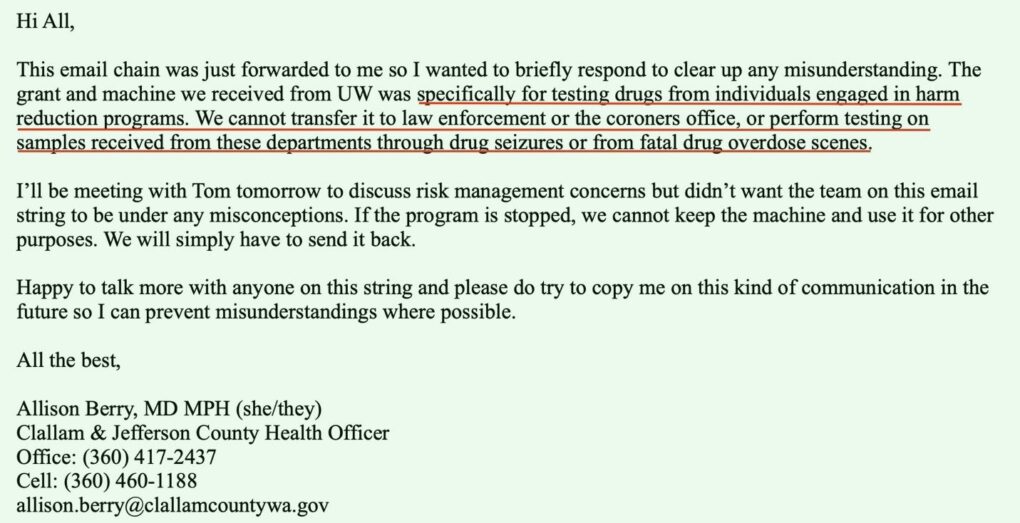
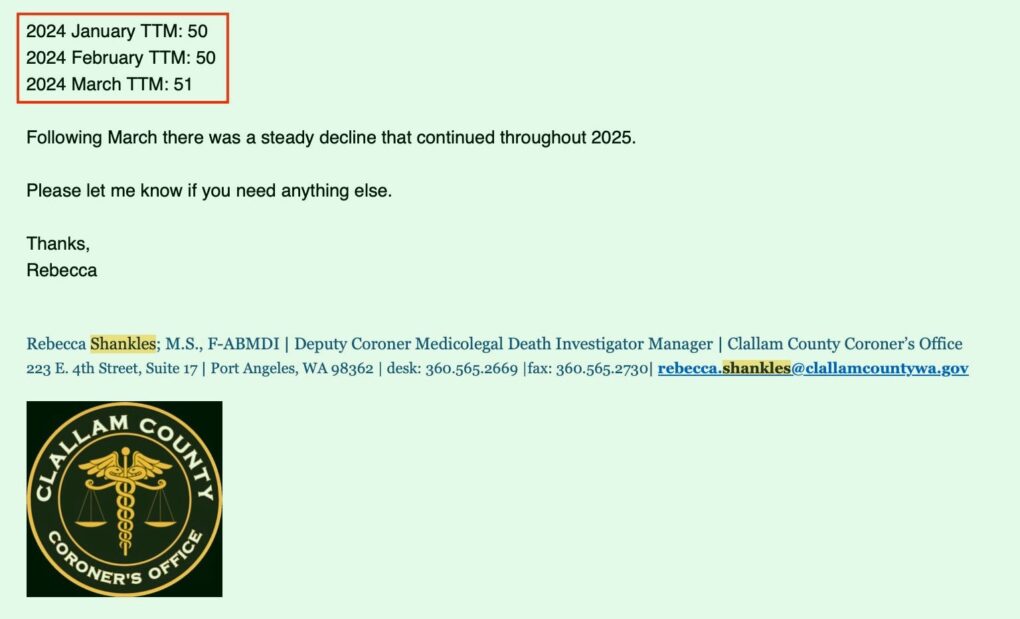
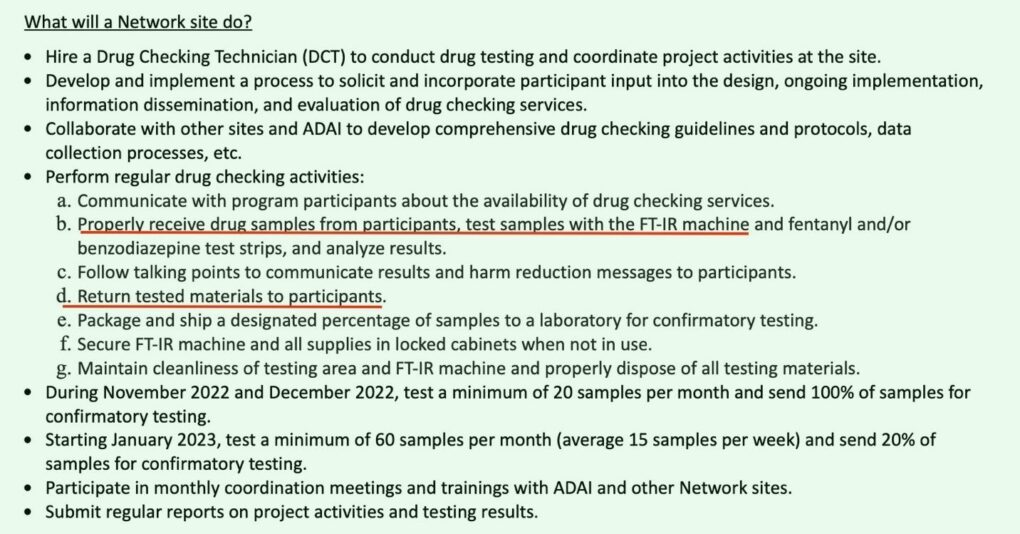
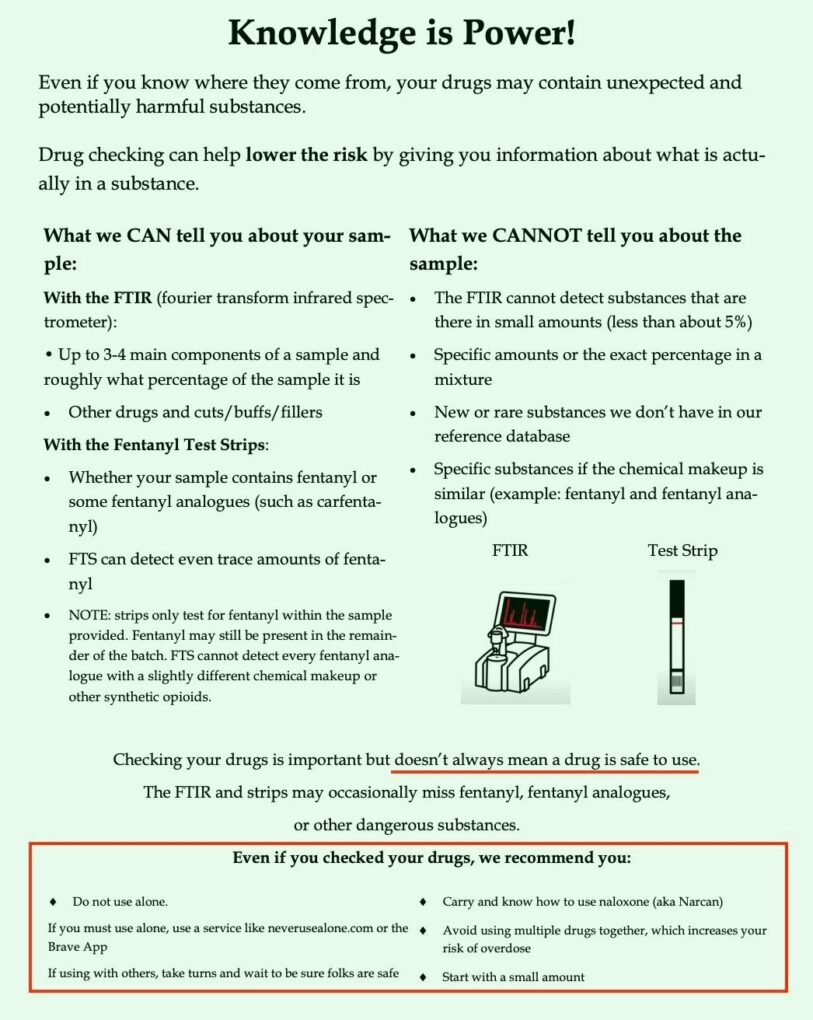
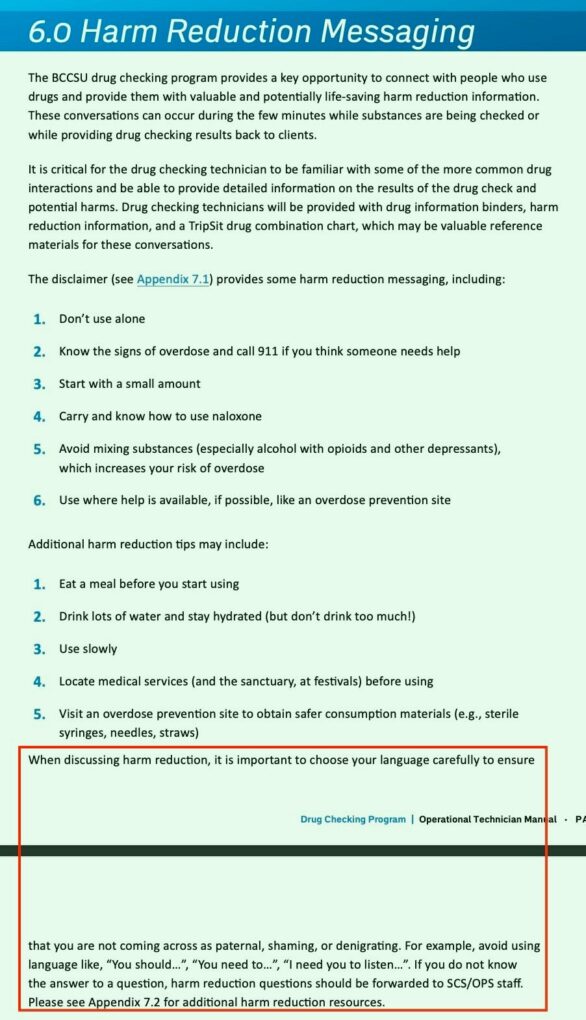
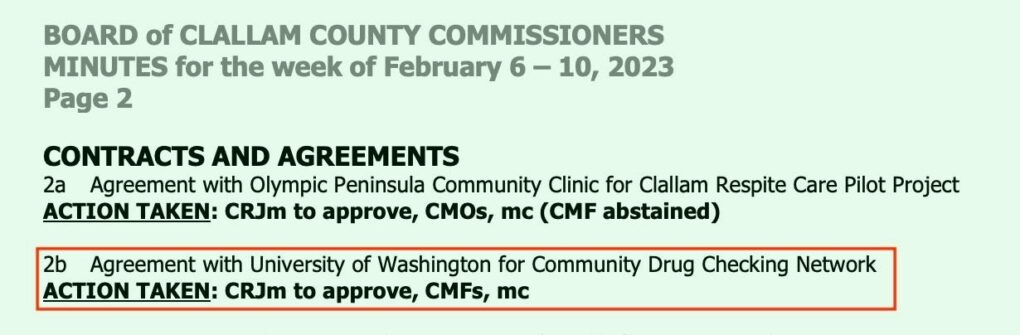
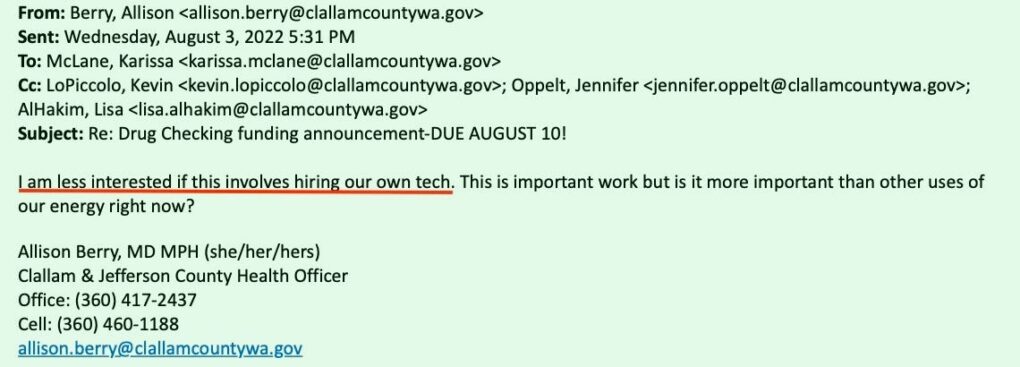
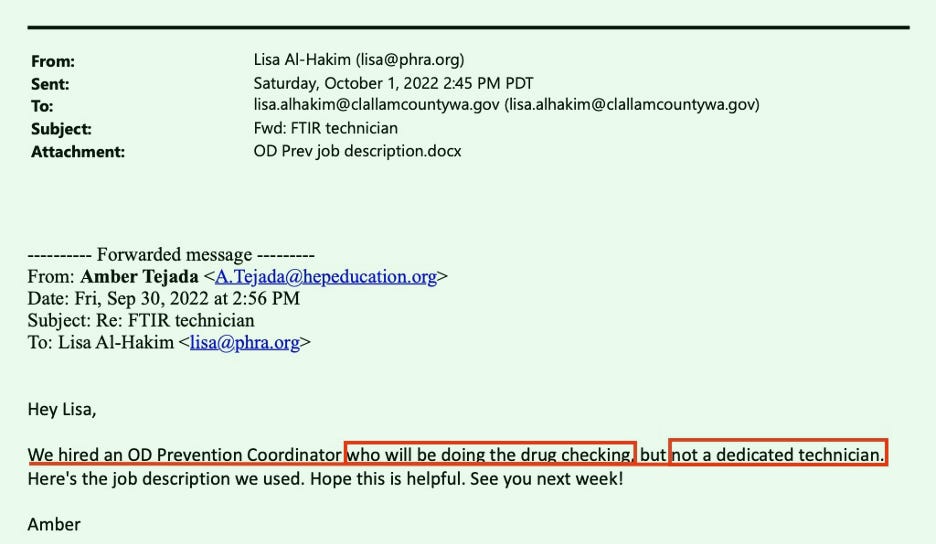
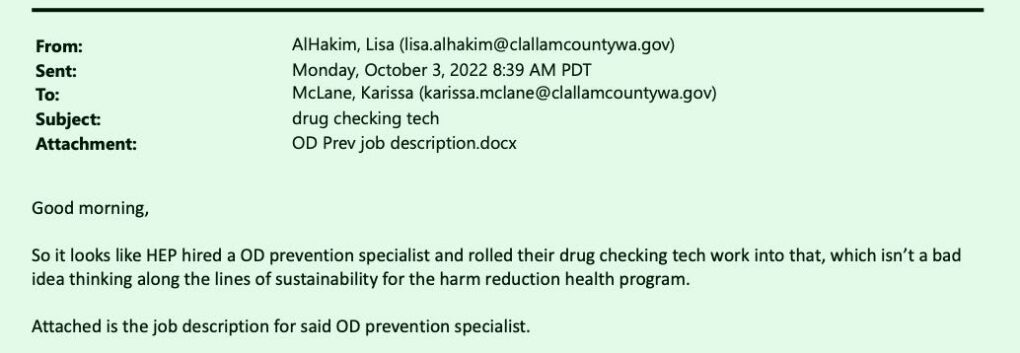
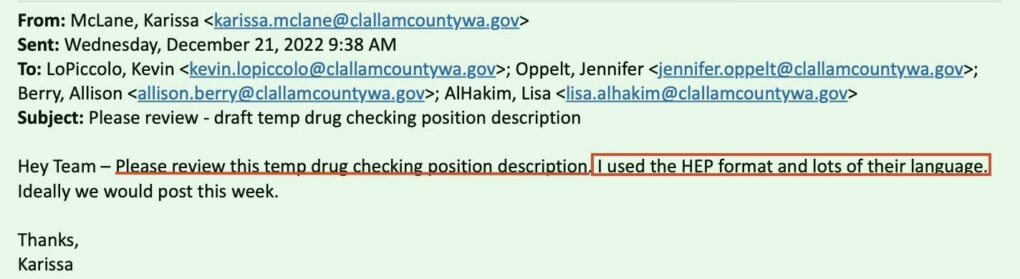
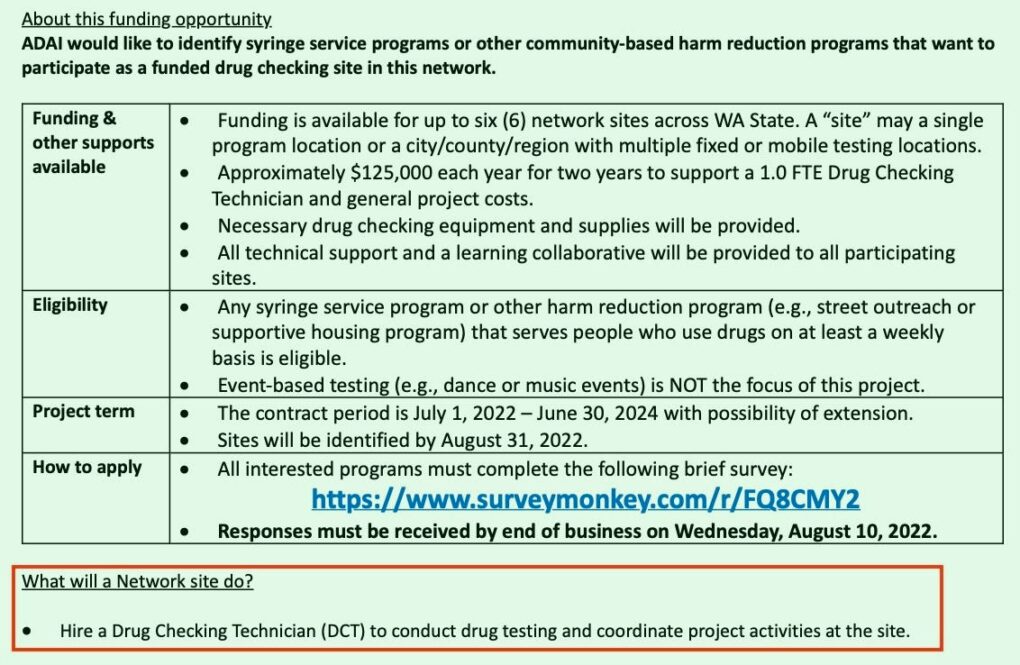
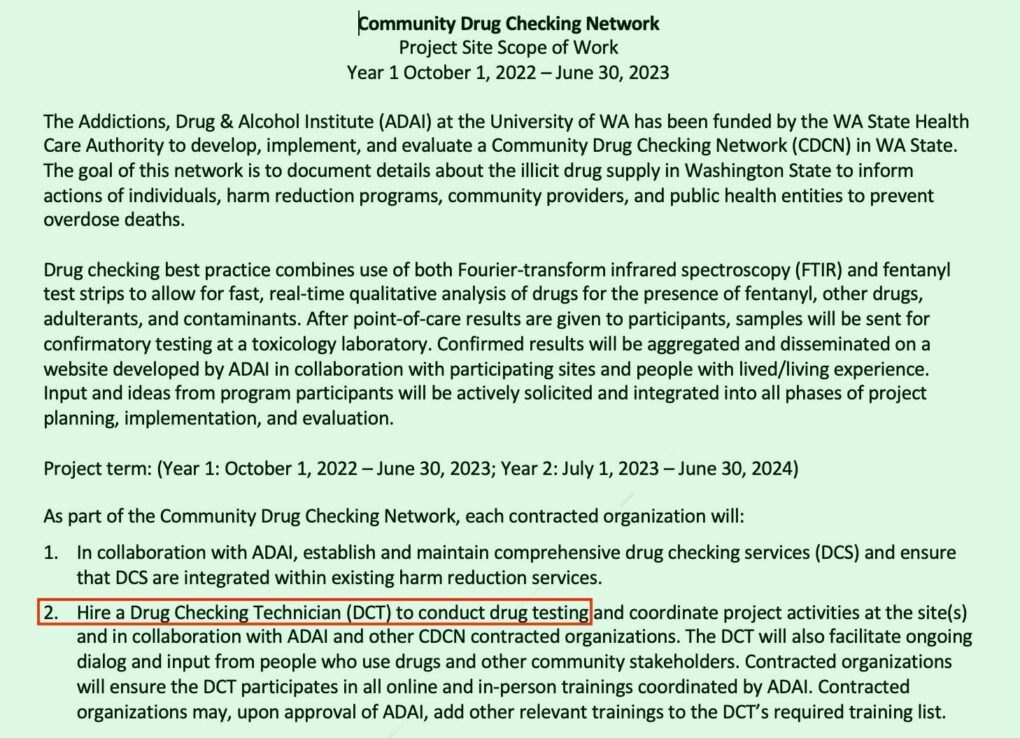
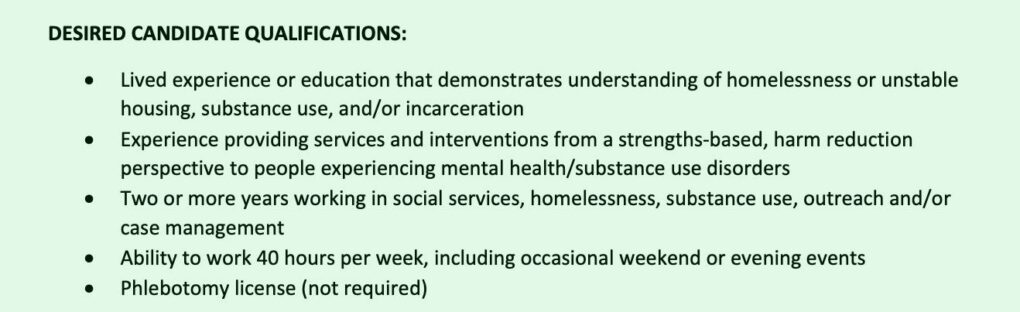
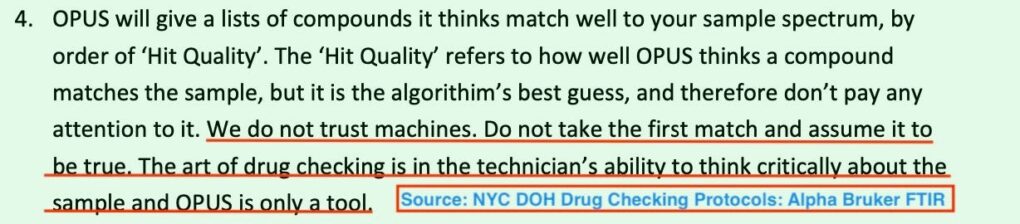
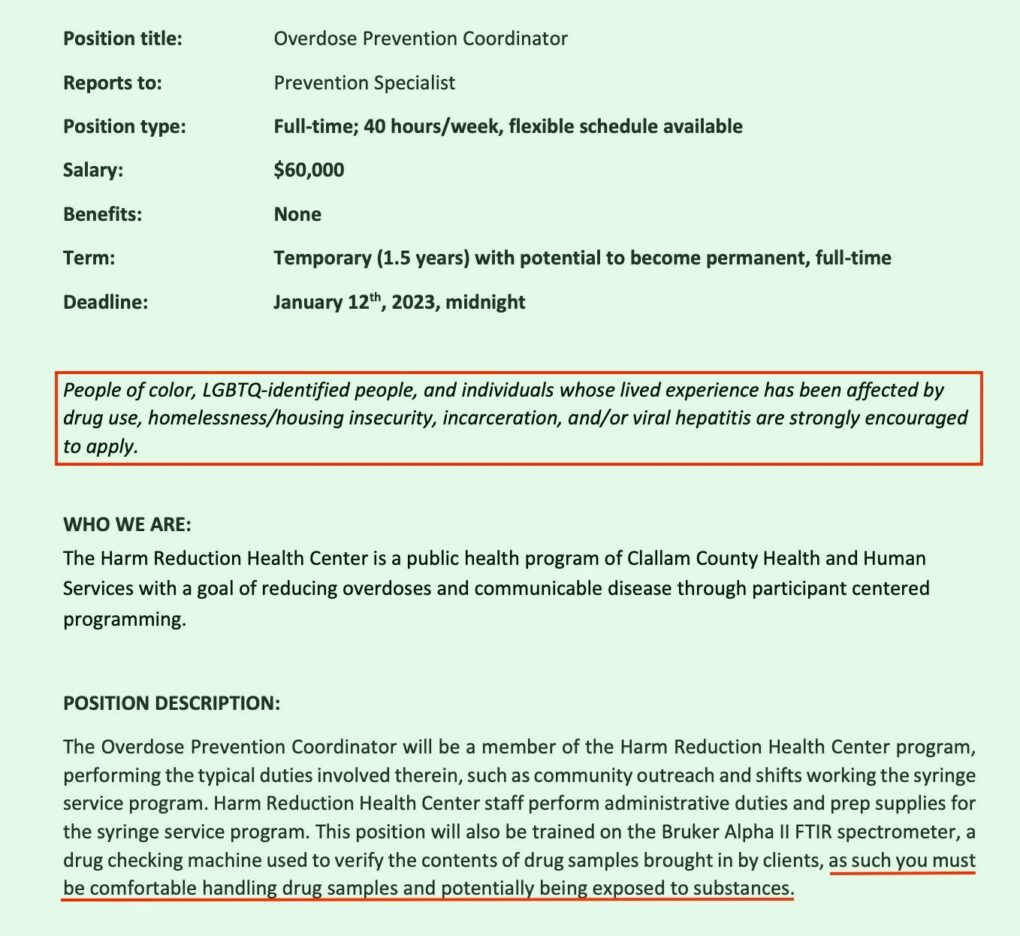
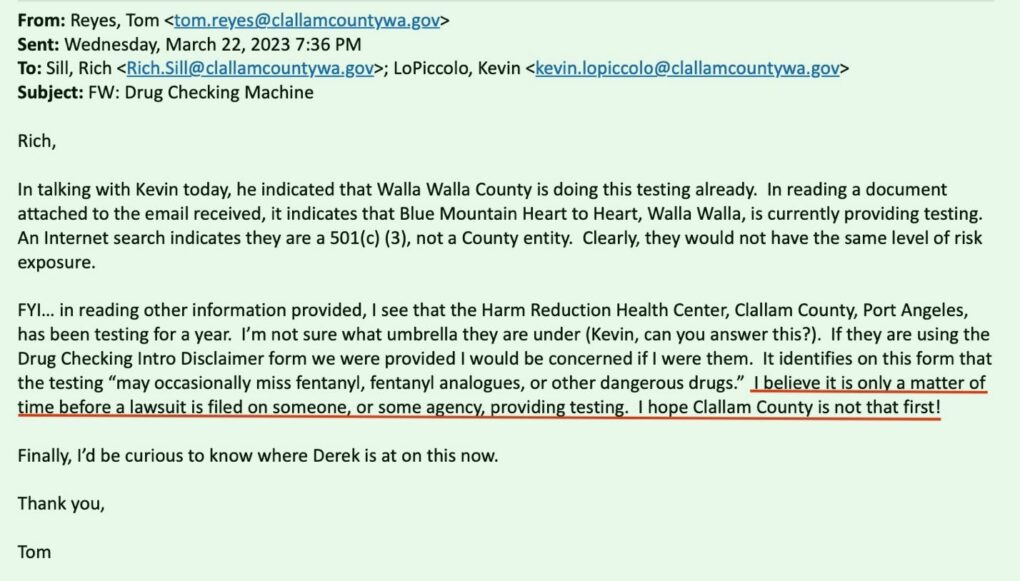
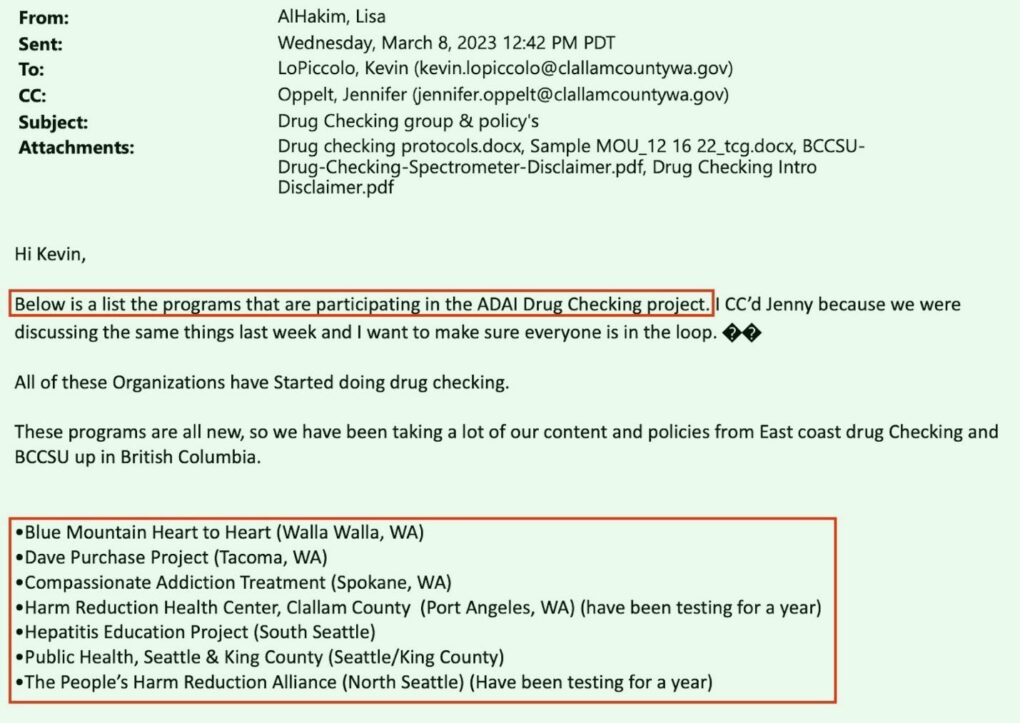
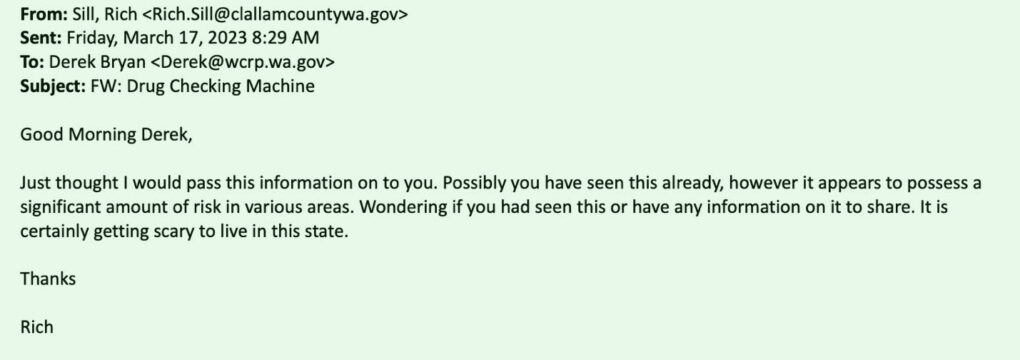
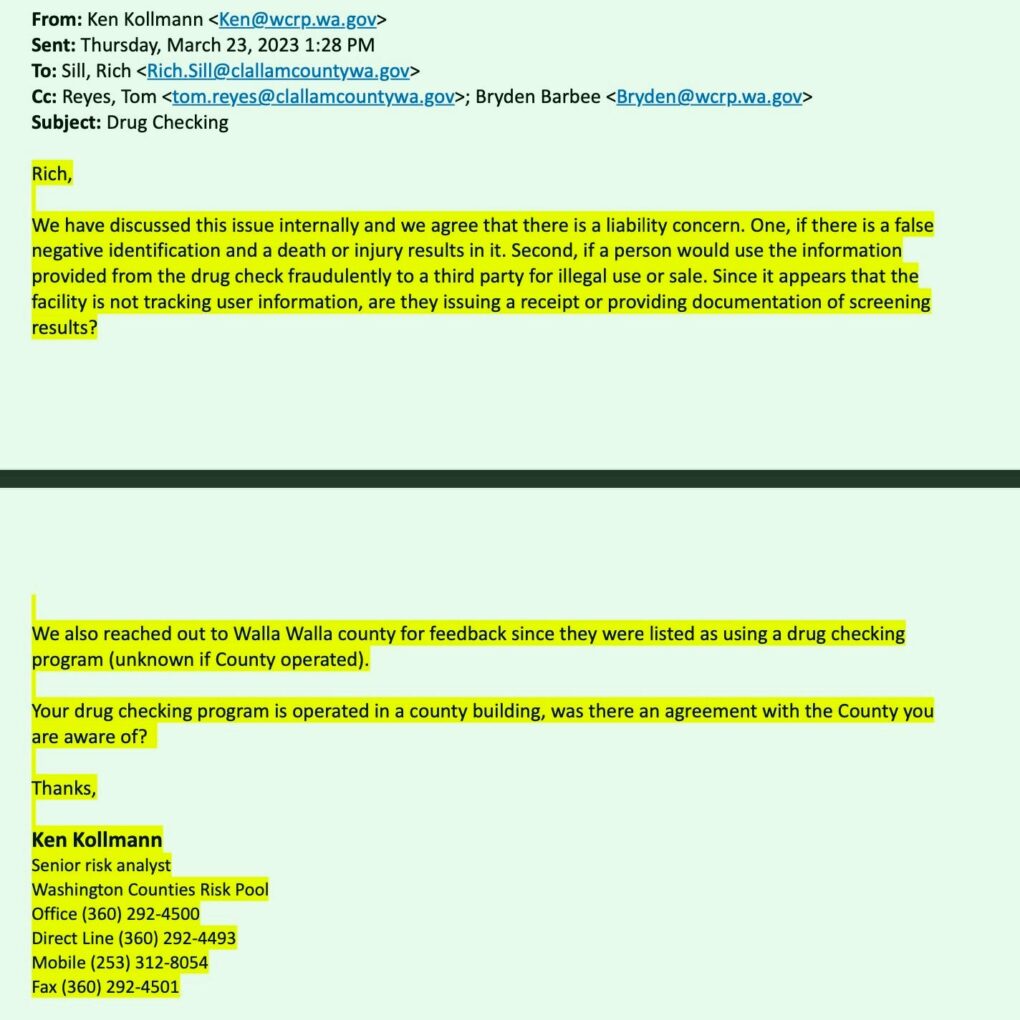
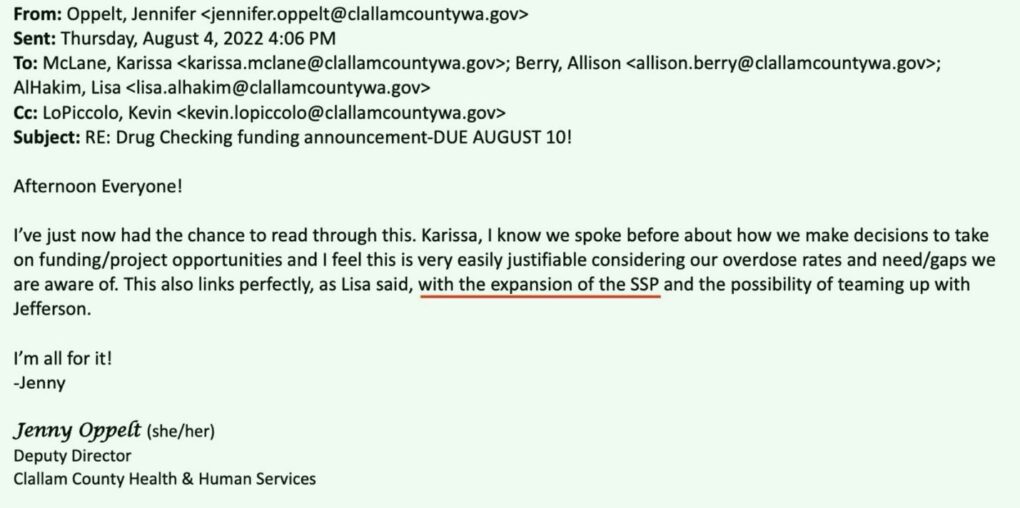
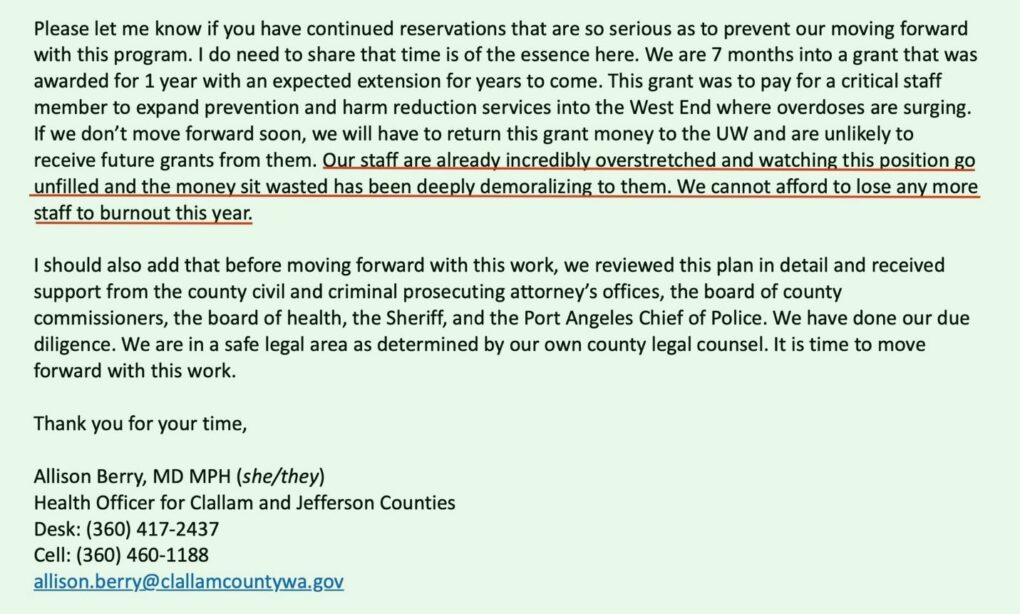
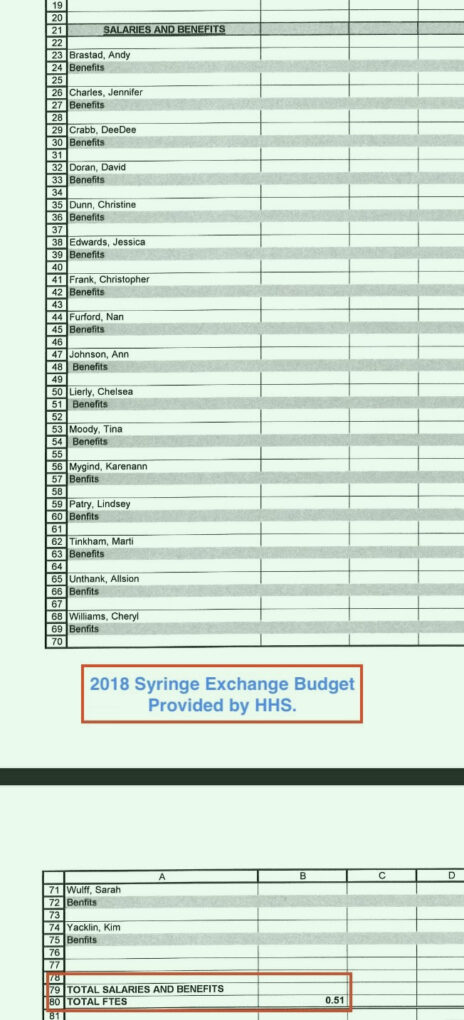
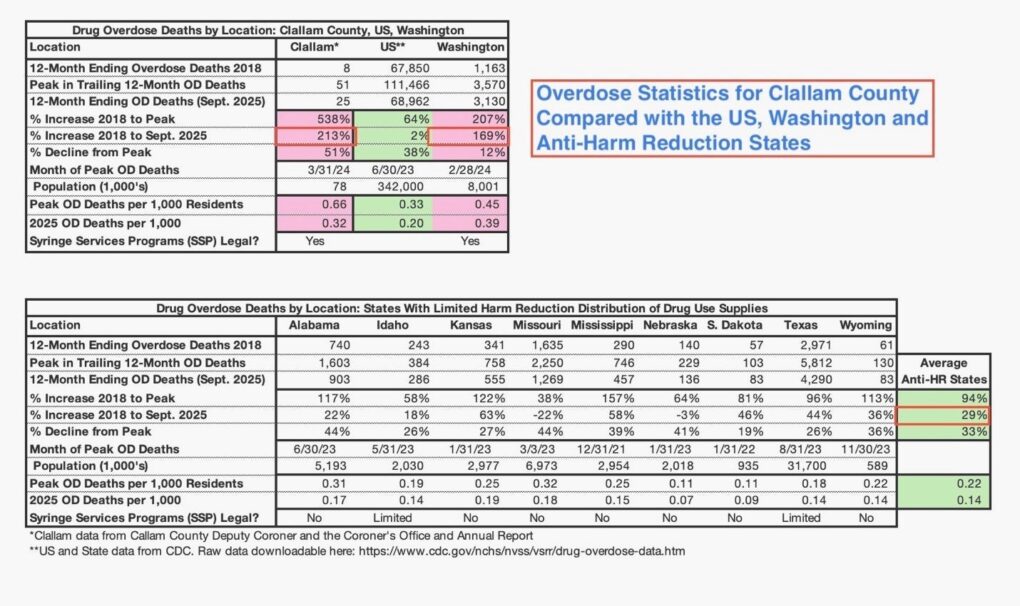
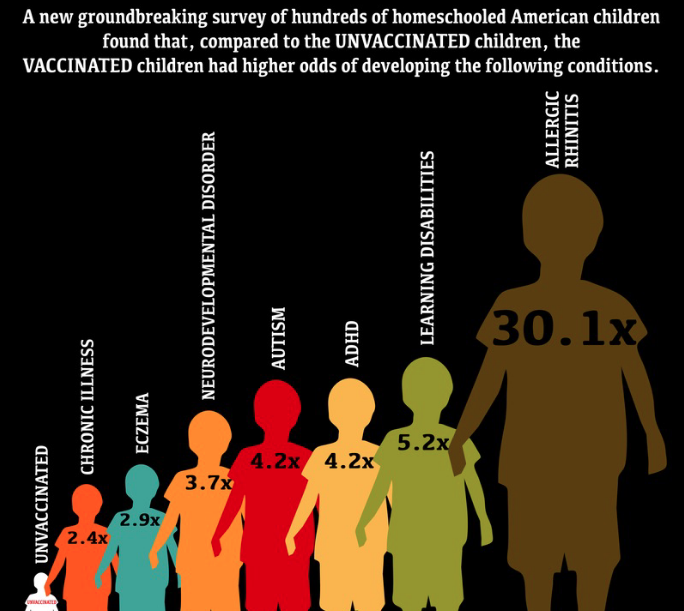
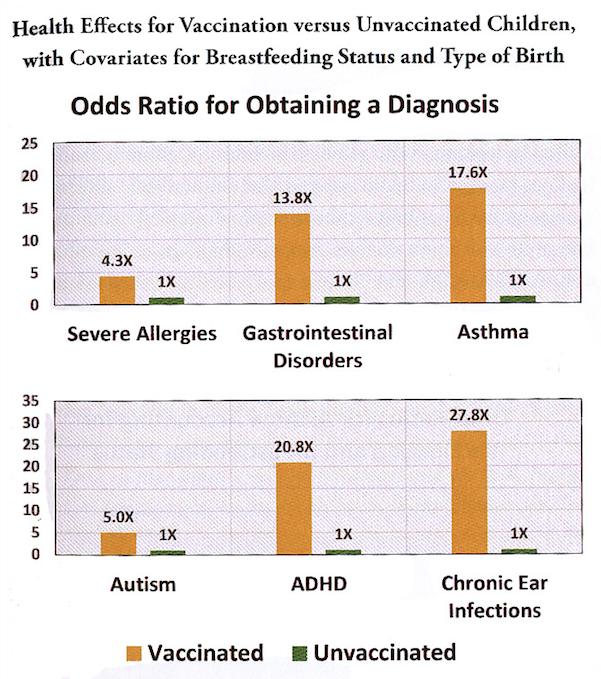
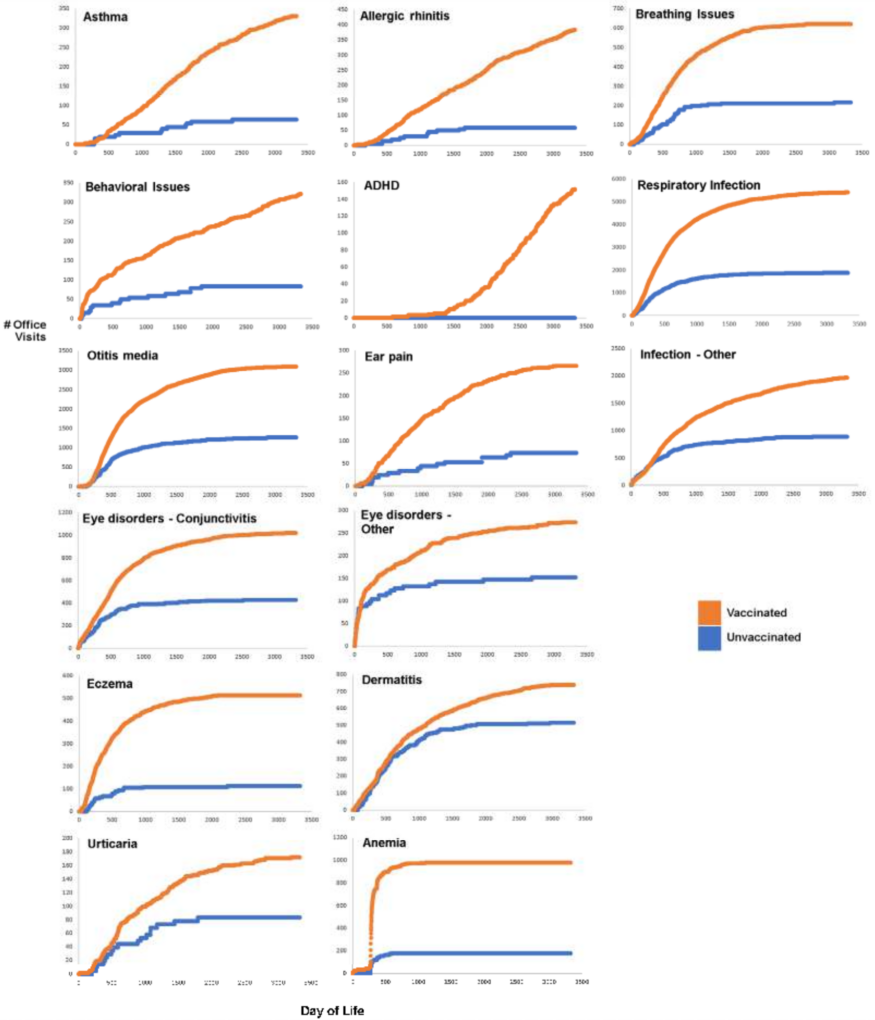
 Unable to convince Zervos to publish the study, Del Bigtree/ICAN tells the story in a powerful documentary, An Inconvenient Study. Released in October 2025, and winner of Best Film at the Malibu Film Festival, it is as much a tale of a medical system that demands adherence to its orthodoxy as it is a film shattering the myth that vaccines make kids healthier. Watch it
Unable to convince Zervos to publish the study, Del Bigtree/ICAN tells the story in a powerful documentary, An Inconvenient Study. Released in October 2025, and winner of Best Film at the Malibu Film Festival, it is as much a tale of a medical system that demands adherence to its orthodoxy as it is a film shattering the myth that vaccines make kids healthier. Watch it 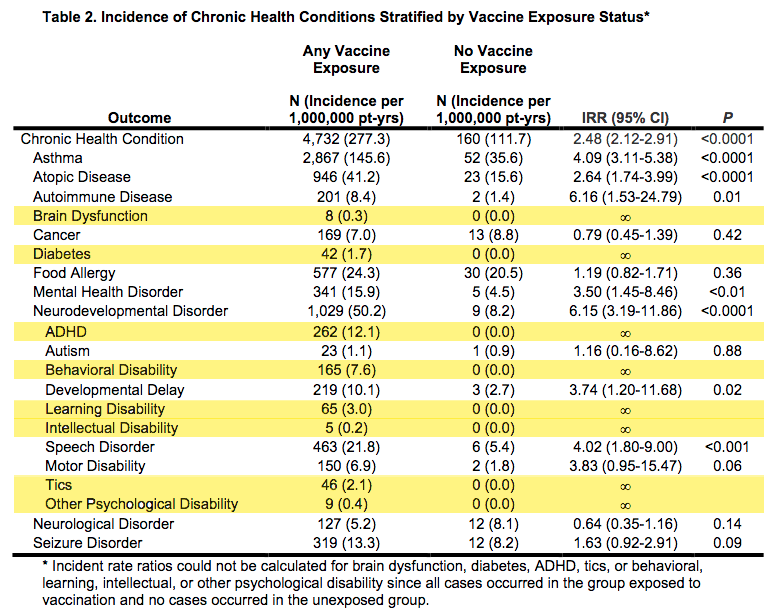
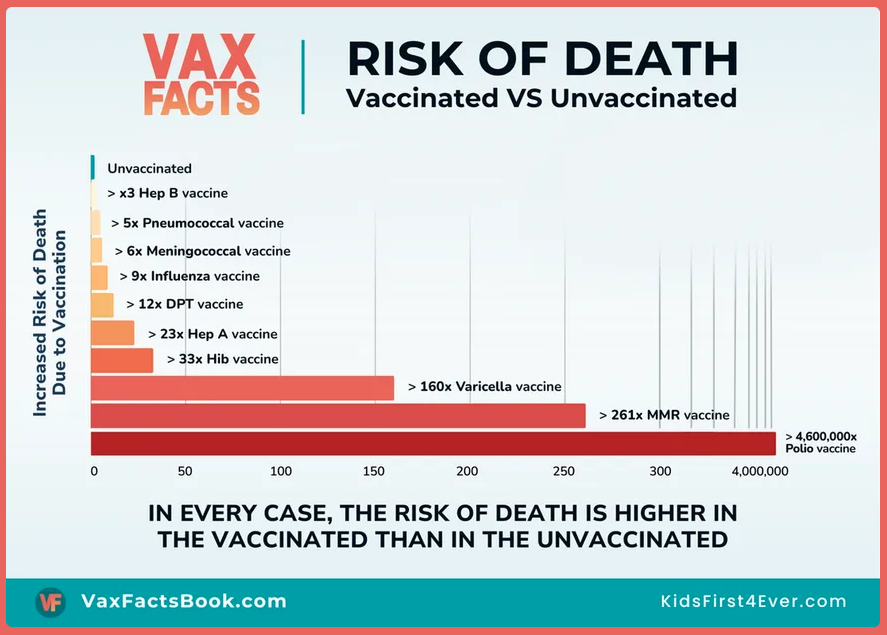
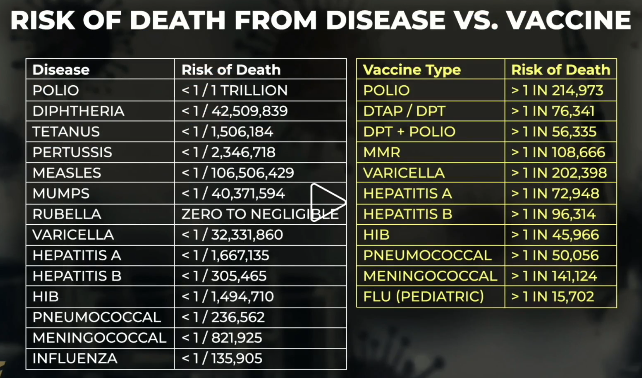
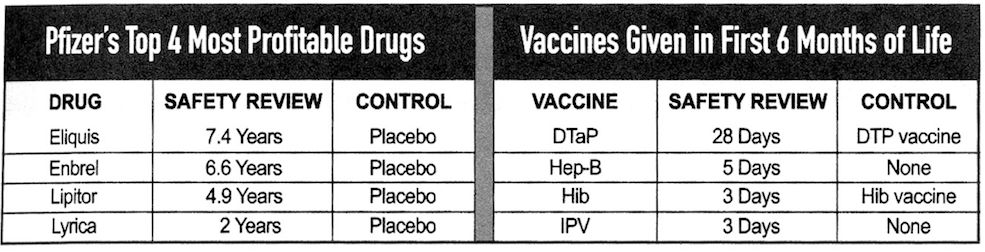
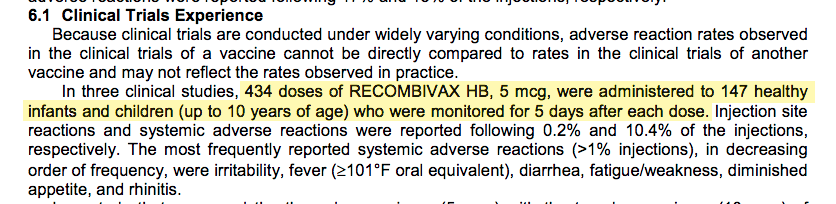
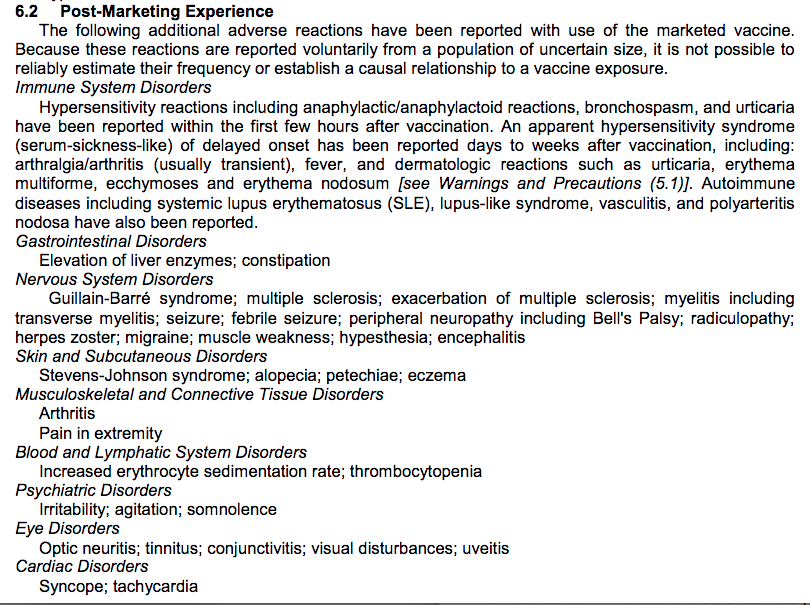
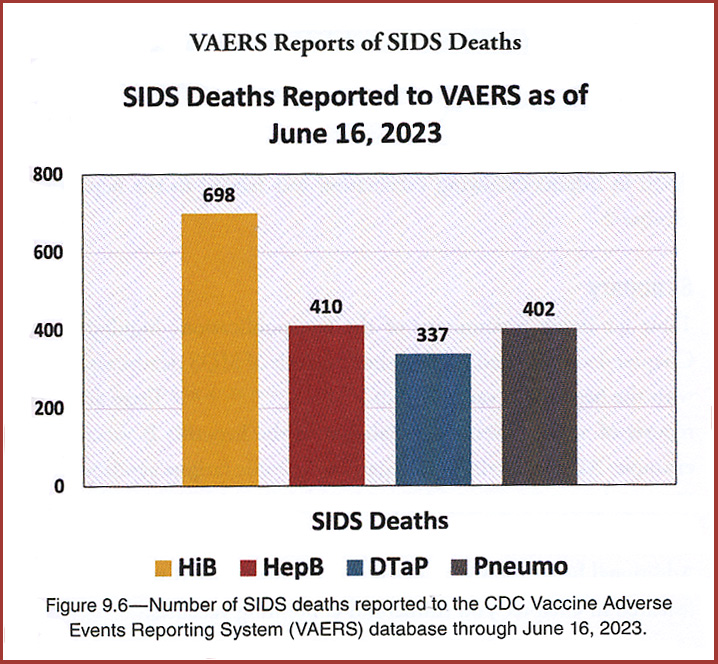
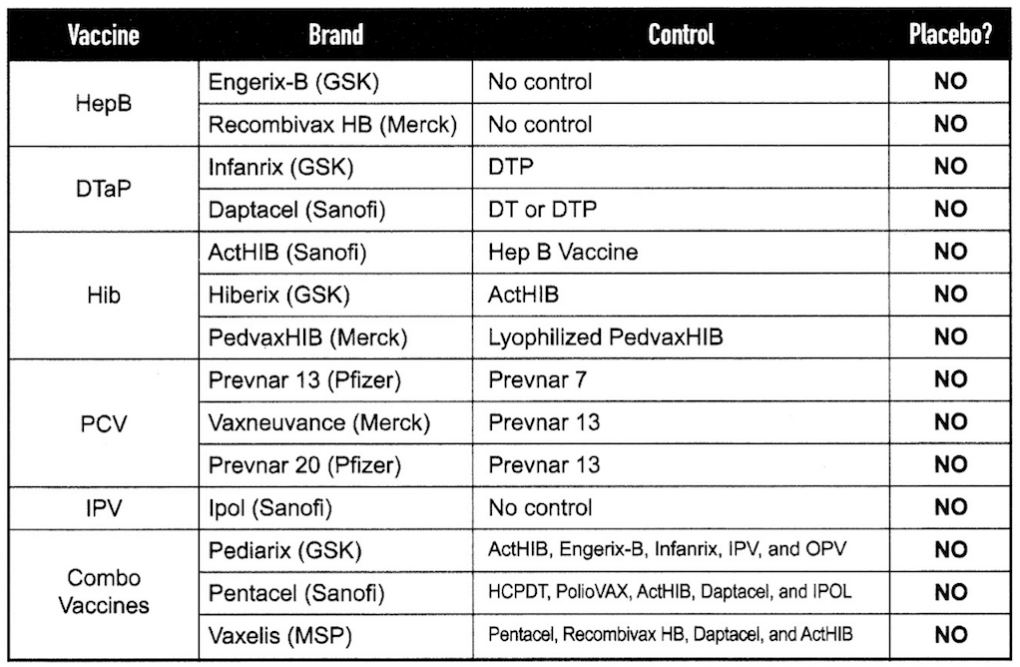
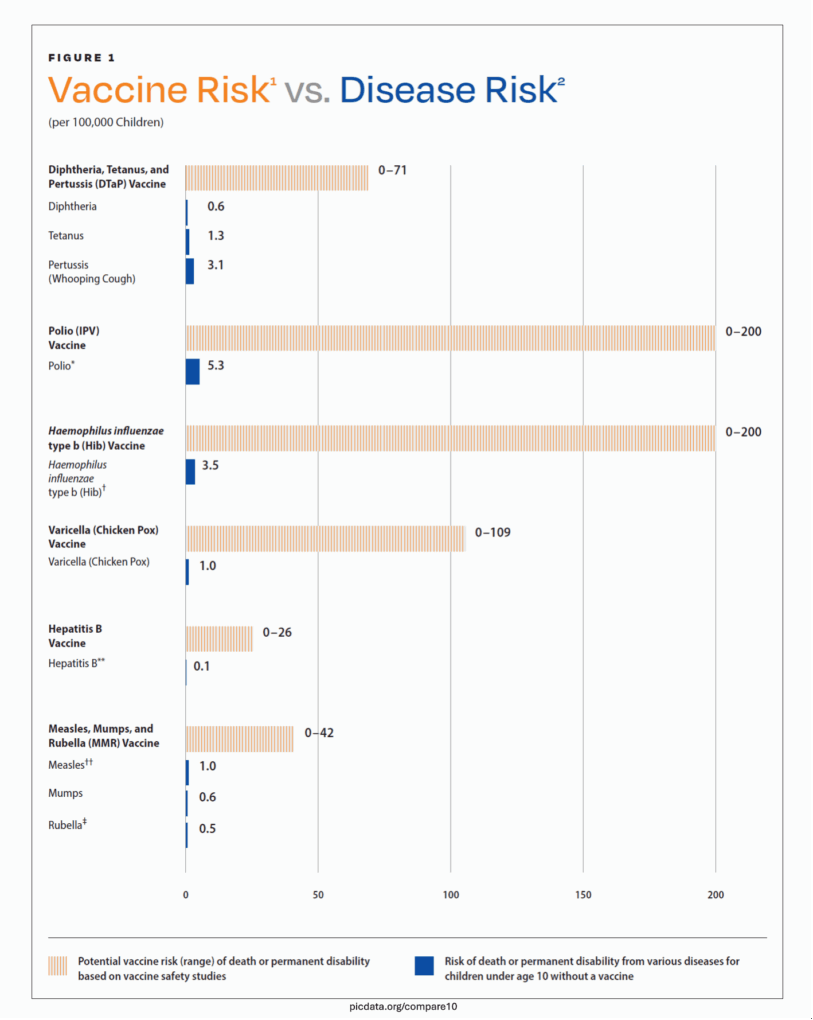
 The number of pediatricians refusing to care for children who do not adhere to the full CDC schedule is considerable. A
The number of pediatricians refusing to care for children who do not adhere to the full CDC schedule is considerable. A 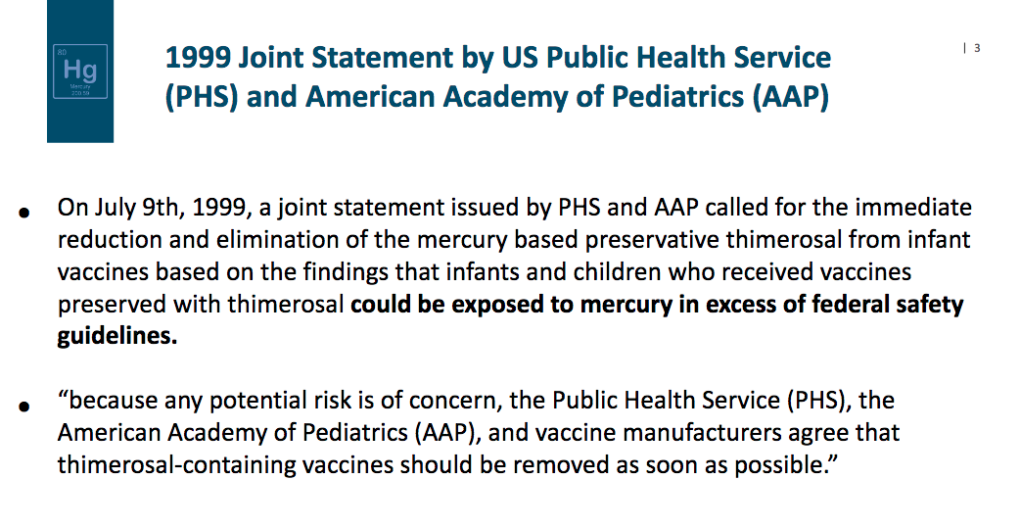
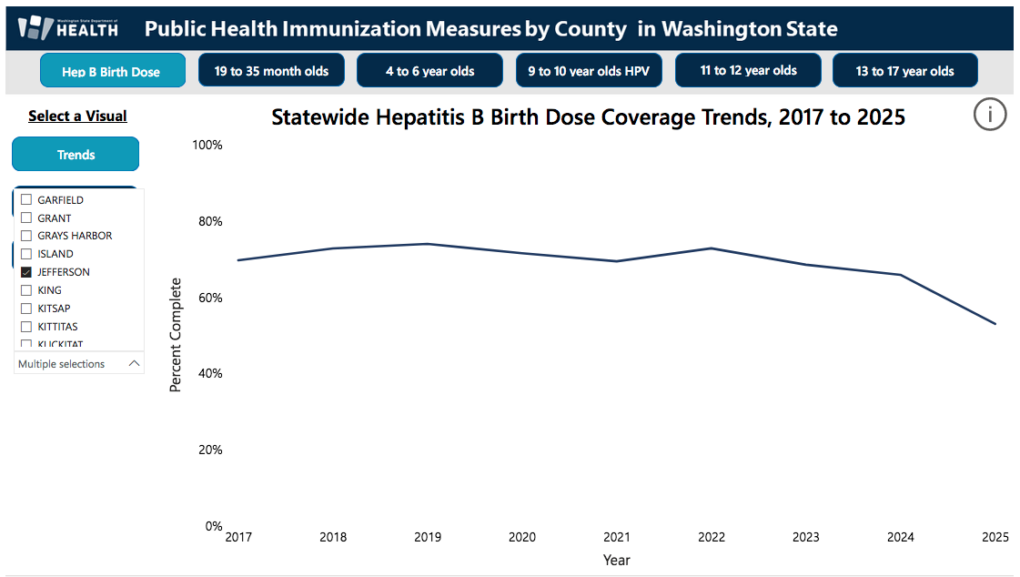
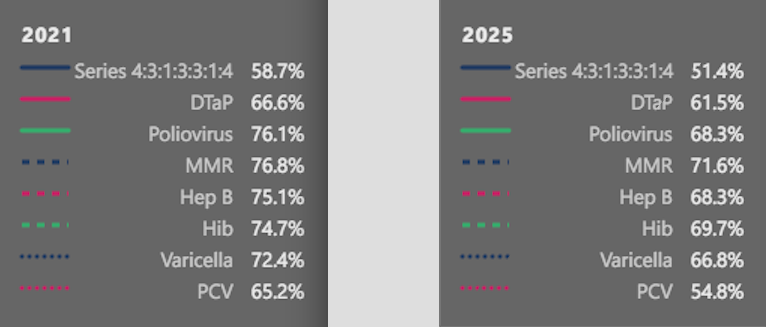
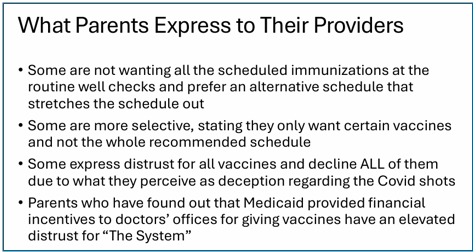
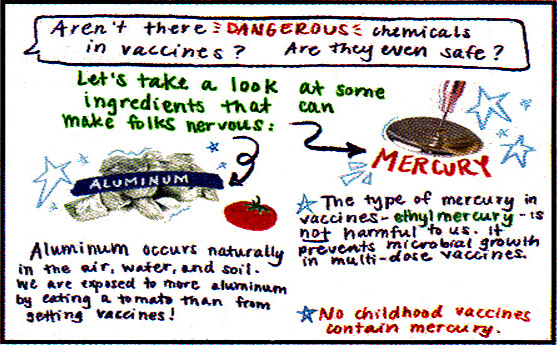
 This fraud was the subject of the shocking and controversial movie
This fraud was the subject of the shocking and controversial movie  Bowing to the pressure, in 1986 Congress removed all liability from drug companies for childhood vaccines they produced. This get-out-of-jail-free card, eliminating industry responsibility for safety, was unprecedented.
Bowing to the pressure, in 1986 Congress removed all liability from drug companies for childhood vaccines they produced. This get-out-of-jail-free card, eliminating industry responsibility for safety, was unprecedented.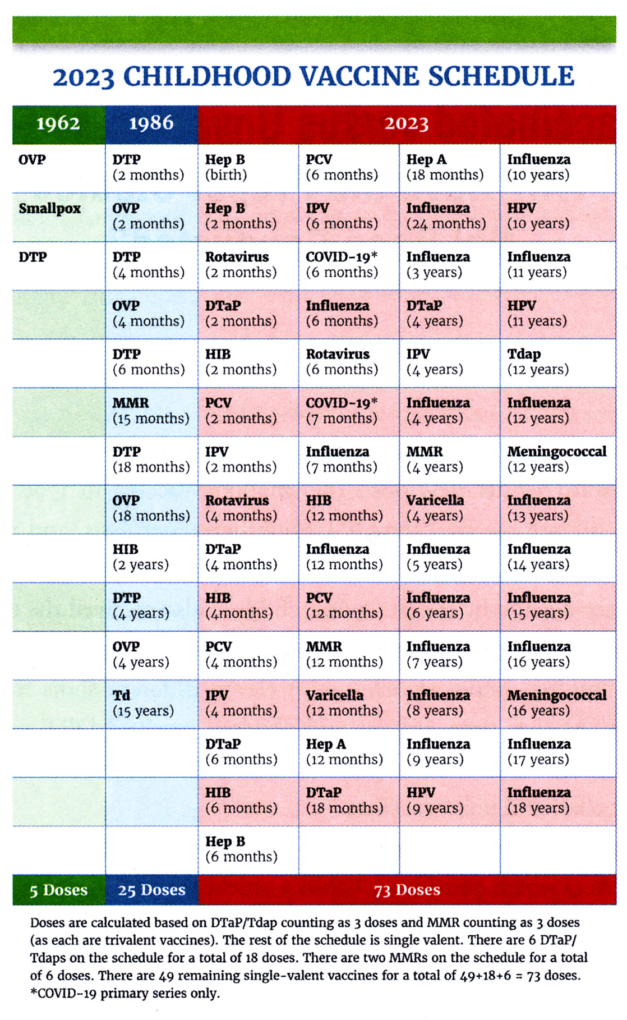
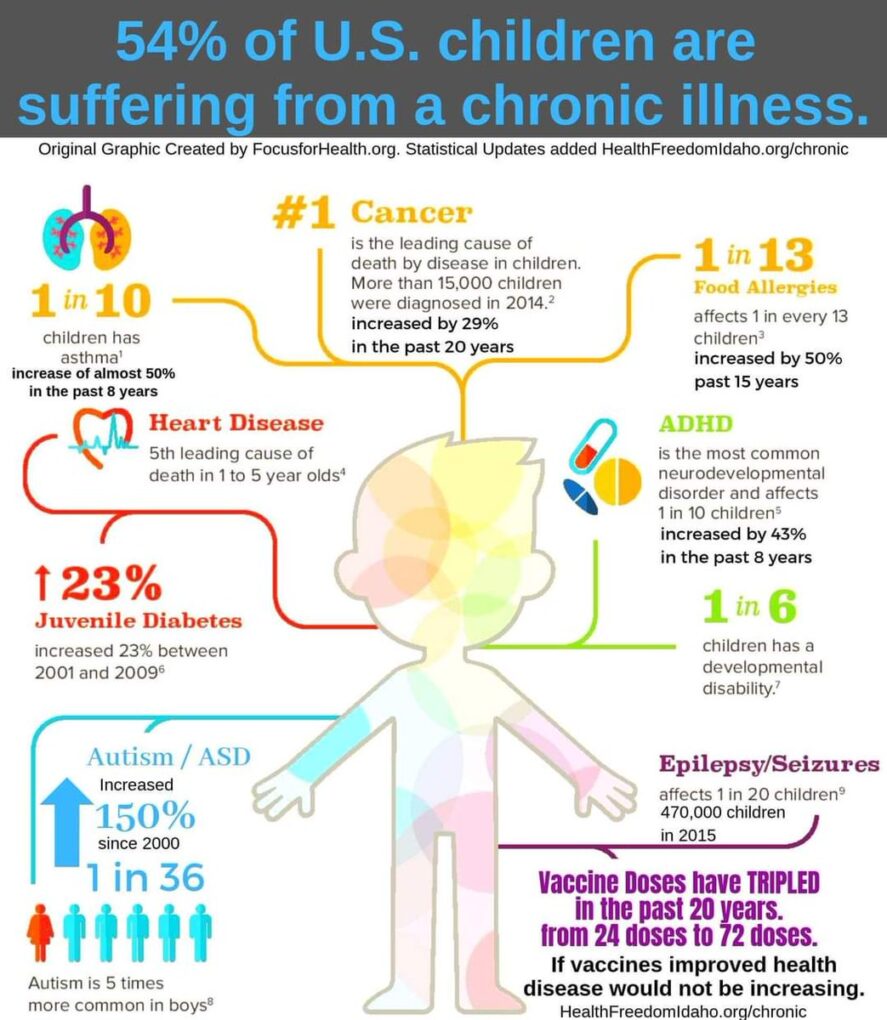
 Traveling to every U.S. state on the continent, its dedicated team video-taped thousands of stories of vaccine injury and death. More than 8,000 names were signed on the bus’ exterior of adults and children injured or killed by vaccines.
Traveling to every U.S. state on the continent, its dedicated team video-taped thousands of stories of vaccine injury and death. More than 8,000 names were signed on the bus’ exterior of adults and children injured or killed by vaccines.
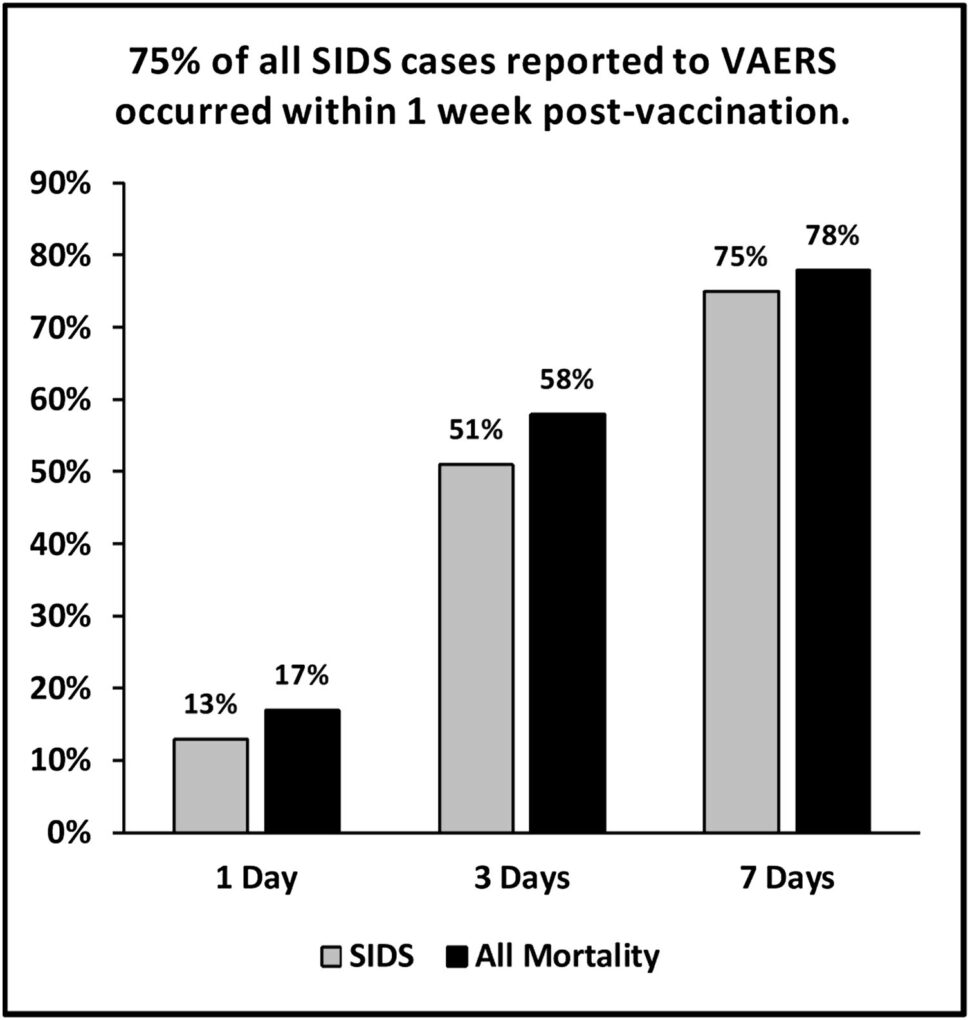
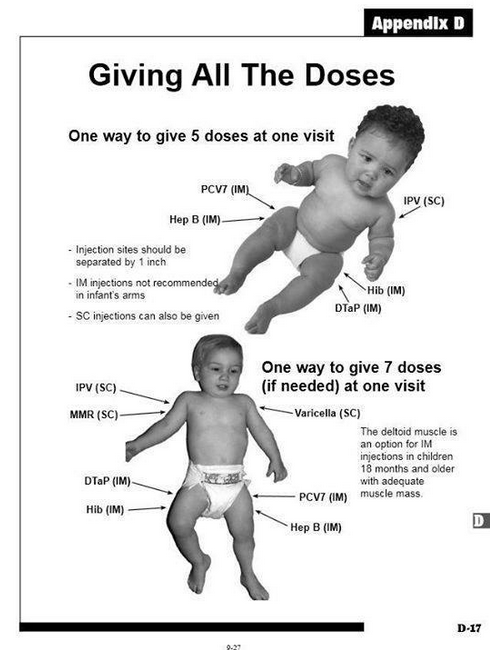
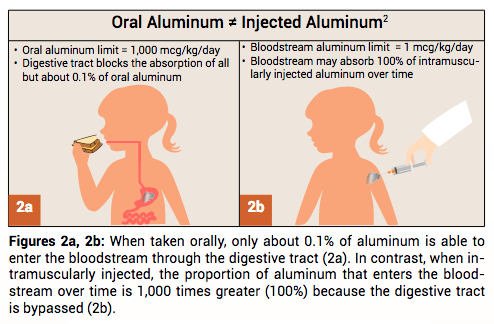
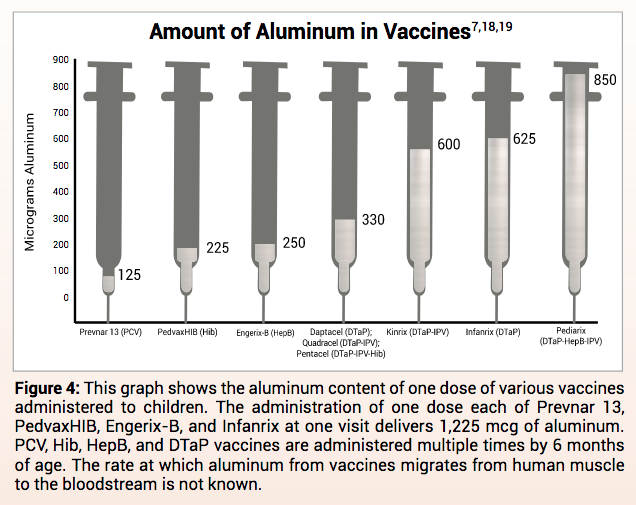
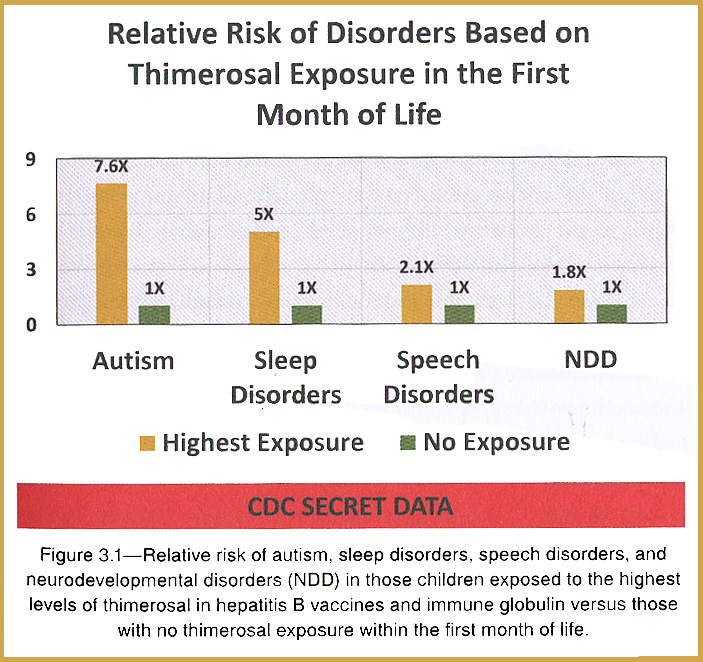
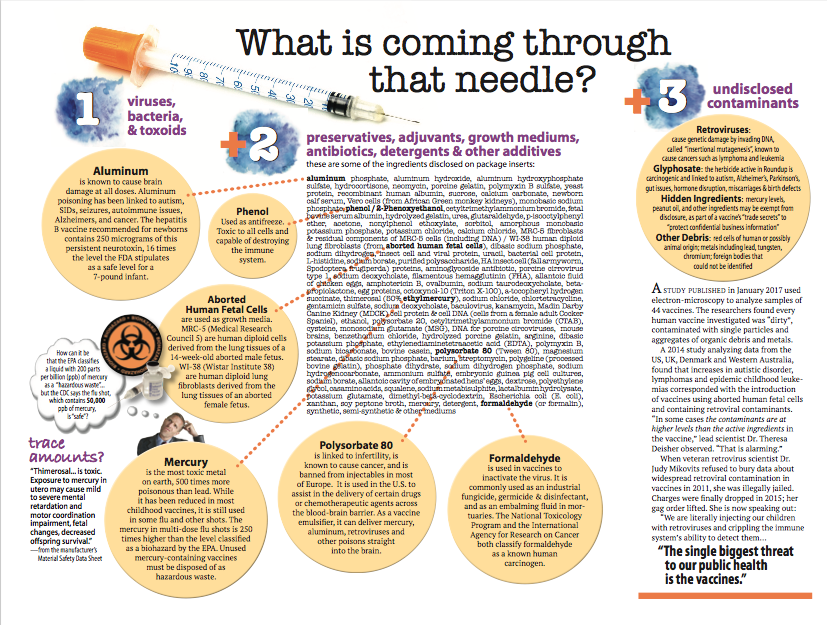
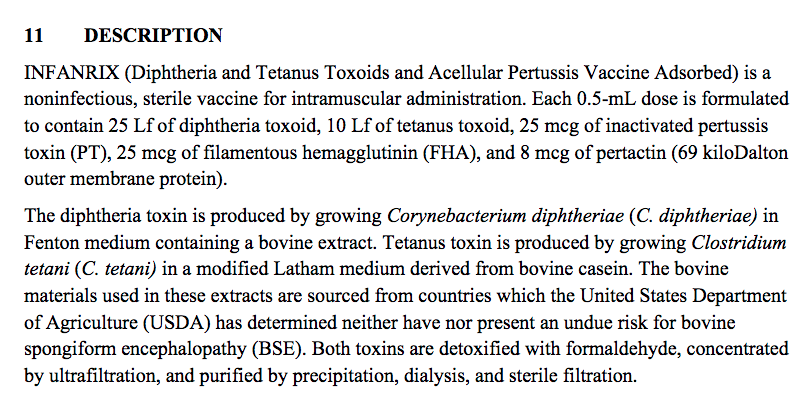

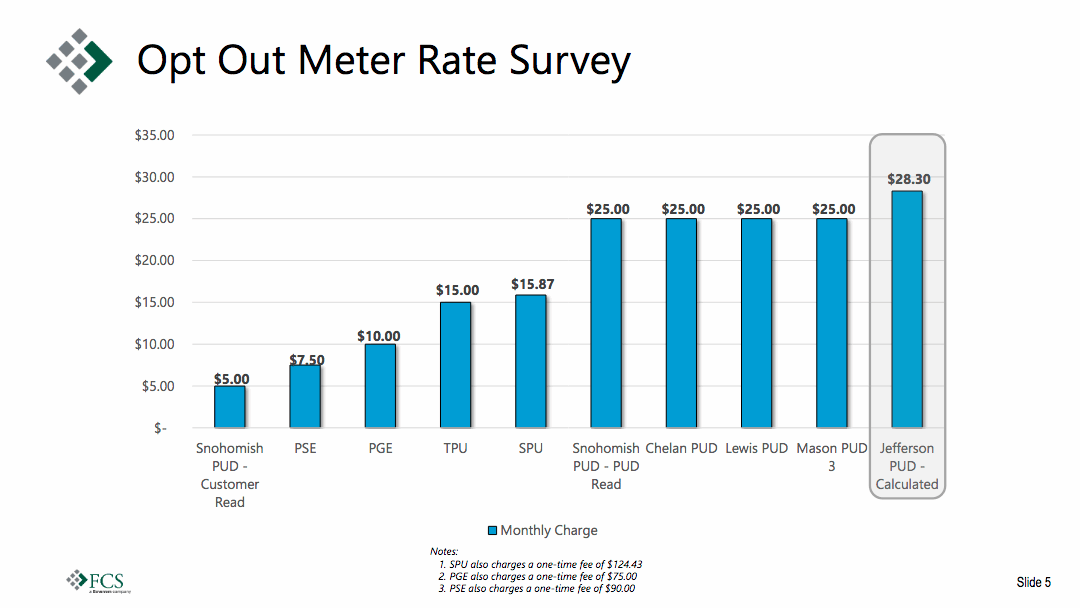
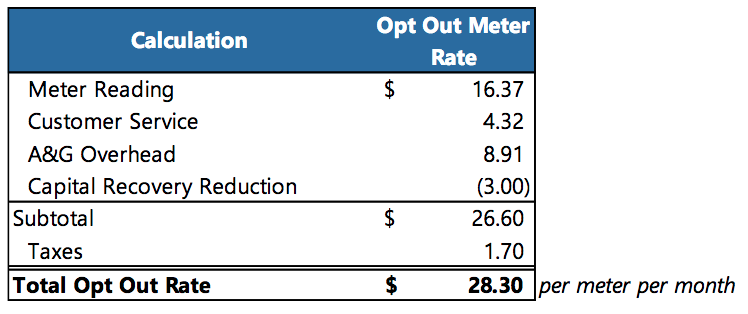
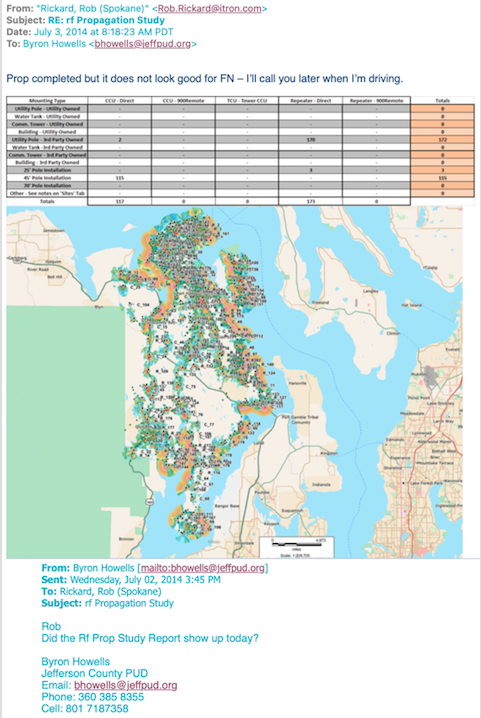
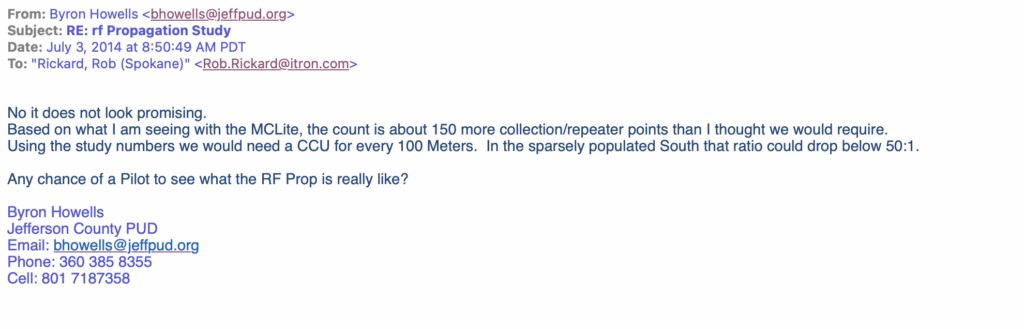
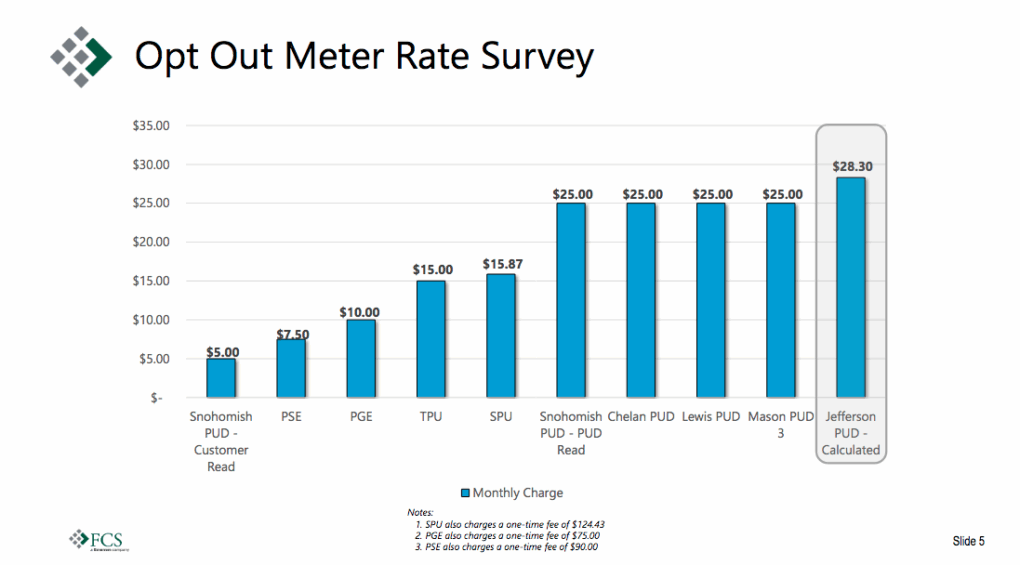
 Simple. Easy. Snap a photo once a month, submit it electronically.
Simple. Easy. Snap a photo once a month, submit it electronically.


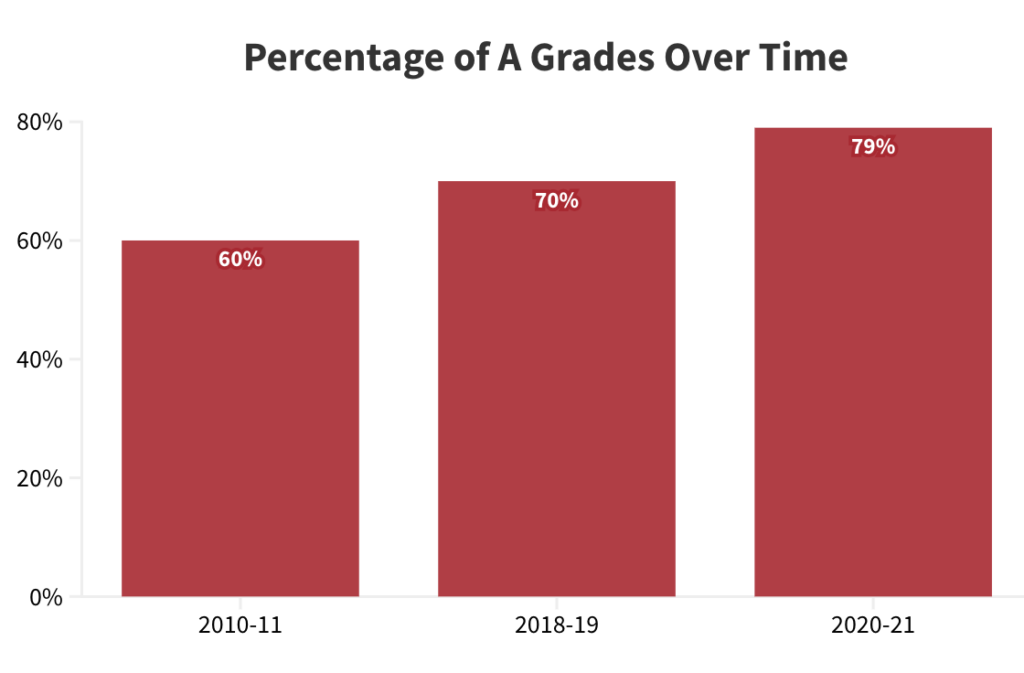

{kind=link}
{kind=link}