by Stephen Schumacher | Jan 30, 2021 | General
Amid calls to double-down on mask requirements with “100 days of masking”, the real news is the latest research confirming the ineffectiveness and dangers of masking against viruses.
On Nov. 18 was unveiled the first-and-only real-world, randomized, controlled trial “to assess whether recommending surgical mask use outside the home reduces wearers’ risk for SARS-CoV-2 infection”, concluding “the difference observed was not statistically significant” between the masked and control groups.
This Danish study is the lead evidence cited by the World Health Organization in its new Dec. 1 guidance on “Mask Use in the Context of COVID-19” section “Evidence on the protective effect of mask use in community settings,” stating “a large randomized community-based trial in which 4862 healthy participants were divided into a group wearing medical/surgical masks and a control group found no difference in infection.”
WHO then cited a review of nine other trials finding that “wearing a mask may make little or no difference to the prevention of influenza-like illness”, along with a few studies that “could be considered to be indirect evidence for the use of masks.” WHO concludes “at present time there is only limited and inconsistent scientific evidence to support the effectiveness of masking of healthy people in the community to prevent infection with respiratory viruses, including SARS-CoV-2.”
According to the BBC’s 2019 British Journalism Award-winning medical correspondent Deborah Cohen, “we had been told by various sources WHO committee reviewing the evidence had not backed masks but they recommended them due to political lobbying. This point was put to WHO [which] did not deny.”
Regarding “the efficacy of community-based use of face masks” to protect others, two systematic reviews by the World Health Organization in 2019 and Centers for Disease Control in February, 2020 found “no significant reduction in influenza transmission with the use of face masks.” See also CDC Emerging Infectious Disease Journal, May 2020 (limited efficacy of nonpharmaceutical measures, such as masking, in preventing virus transmission).
But why are masks so ineffective against viruses? Electron micrographs show the size of the SARS-CoV-2 virus is between 0.06 and 0.14 microns. By contrast, standard cloth face coverings and masks have 2.5 micron pore size, with area 625 times bigger than a virus, which is like trying to stop mosquitos using wide-mesh wire fences. Only true surgical masks have near-viral filter pore sizes, but tests show even they let through 12% to 45% of viral-size particles.
More critical than pore size are two other issues impacting mask effectiveness. The first is that surgical masks may be good at stopping bacterial droplets, but viral droplets quickly “evaporate into ‘droplet nuclei’, remain suspended in air for significant periods of time and could be inhaled.” Bar-On, et. al, National Institutes of Health, NCBI Resources, April 2, 2020.
OSHA’s Fact Sheet on Respiratory Infection Control makes clear that “Surgical masks are not designed or certified to prevent the inhalation of small airborne contaminants. … Surgical masks are not designed to seal tightly against the user’s face. During inhalation, much of the potentially contaminated air can pass through gaps between the face and the surgical mask and not be pulled through the filter material of the mask.”
Anyone wearing glasses knows the truth of this, since fogged glasses prove exhalation is flowing up around the nose past the eyes into the air stream… meanwhile coating contact lenses or glasses with germs so they become point sources of infection. Face shields get a bad rap for allowing air to flow around edges, but vape cloud videos show aerosols likewise follow the path of least resistance through the sides and top of surgical masks.
The other critical problem with mask use outside controlled clinical settings is that even when a mask succeeds in catching viruses these do not disappear from existence but instead turn the mask into an active point source of infection. Viruses collected on the mask get regularly dislodged into the air or pushed through the mask by future inhalations and exhalations or touched by hands, potentially infecting the wearer and others. The net effect may be worse than wearing no mask at all.
WHO lists a wide range of other “disadvantages of mask use by healthy people” including “headache and/or breathing difficulties”, “development of facial skin lesions, irritant dermatitis”, “difficulty with communicating clearly”, “discomfort”, “a false sense of security”, “improper mask disposal”, “environmental hazards”, along with special difficulties for “children, developmentally challenged persons”, “those with asthma or chronic respiratory or breathing problems”, etc.. See also, “Full Time Mask Wearing Brings Its Own Problems,” The Crimson White, University of Alabama, August 20, 2020.
Neurosurgeon researcher Dr. Russell Blaylock warns that reduction in blood oxygenation from prolonged mask wearing is “associated with an impairment in immunity” with “an increased risk of infections … including COVID-19 and making the consequences of that infection much graver”, as well as promoting “spread of cancers”, “cardiovascular (heart attacks) and cerebrovascular (strokes) diseases.” Continually rebreathing moist respiratory wastes beneath a mask raises the concentration of any viruses in the lungs and nasal passages causing worse reactions. “Newer evidence suggests…by wearing a mask, the exhaled viruses will not be able to escape and will concentrate in the nasal passages, enter the olfactory nerves and travel into the brain.”
In conclusion, the best current science does NOT support mask mandates nor claims that increased mask wearing would reduce virus transmission or save lives. The reality is quite the opposite.
[Editor’s note: Mr. Schumacher provided many additional sources beyond those quoted or linked in this article. We link those additional sources below.]
[From Mr. Schumacher: “My thanks to Dr. Roger Koops for his generous correspondence helping sort out evidence relating to mask pore size and surgical mask effectiveness, and especially for his original insights about how masks can become dangerous point sources of infection.”]
Additional source material (partial citations):
“Environmental Role in Influenza Outbreaks”
“Coronavirus: Mask Wearing Risks Isolating Deaf People”
“Surgical Mask Induced Deoxygenation During Surgery”
“Hypoxia Inducible Factor-1 Negatively Regulates Th1 Function”
“Hypoxia Enhances Immunosuppression”
“Hypoxia-driven Immunosuppression”
“Immunoexcitatory mechanisms in glioma proliferation” (relating to cancer)
“Nuclear factor-kB” (relating to cancer)
“Chronic Intermittent Hypoxia Induces Artherosclerosis”
Chemical neuroscience of COVID-19 transmission
Nervous system involvement after COVID-19 infection
“Masks for all not based on sound data,” University of Minnesota
“Universal Masking in Hospitals in the COVID Era,” N.E. Journal of Medicine
“Masks are Neither Effective Nor Safe,” Colleen Huber, NMD
“Masks Likely Do Not Inhibit Viral Spread,” Mercola
“Should Everyone Wear a Mask in Public? Maybe–But It’s Complicated,” Forbes
“Mask May Protect Others, But Not You” Forbes
by Craig Durgan | Jan 29, 2021 | General
The currently adopted Jefferson County Comprehensive Plan has the following important statement:
“Even with Jefferson County’s current low growth rate, the shortage of attainable housing is not reconciled. The condition of average housing prices being beyond what average wages can attain has been documented over the last two decades in state and local reports, including the Port Townsend/Jefferson County Housing Action Plan (2006).”
It does not appear that Jefferson County is in compliance with its own Comprehensive Plan. The above-quoted statement confirms that. While the Comprehensive Plan actually encourages affordable housing, its Unified Development Code (UDC) does the opposite, as I will explain.
There are currently many impediments to providing adequate housing for workers, young families, small business owners, artists–just about anybody who doesn’t have tons of money. The most widely-discussed impediment is the lack of a sewer in Port Hadlock. Jefferson County is currently working on that issue, although progress is quite slow.
There are other impediments to building adequate housing that do not receive as much attention, though their impact is just as negative on our housing problem.
Currently the county has a minimum 5 acre subdivision requirement. This means that land can not be subdivided like it used to be. There are over 300 existing subdivisions in Jefferson County. These subdivisions are where the majority of homes are. By restricting the ability to subdivide more property into smaller than 5 acre lots the cost to build goes up dramatically. No one can build a house affordable to an average family on a 5 acre lot. The cost of the land is over $200,000, to start with. If the county permitted realistic subdivisions, a developer could create much smaller, and therefore cheaper lots so that more people could afford the new housing that would be built.
Under Washington regulations the minimum lot size allowed is 12,500 square feet in areas with public water and soils suitable for septic drainage fields. But the county does not allow a subdivision if the parcels are smaller than five acres–period. The result is that there is a severe lack of buildable and affordable lots in Jefferson County. This, in turn, artificially limits the housing supply and drives prices to unaffordable levels. The situation created by our county’s land use regulations, as I have written before, is driving young people out of our communities and turning us into an exclusive retirement community for the wealthy who can afford inflated housing prices.
It would appear that Jefferson County is not following the State-mandated Growth Management Act nor their own Comprehensive Plan. Under the State Growth Management Act the county is required to plan for growth. But Jefferson County regulations are preventing growth.
Something needs to be done to bring Jefferson County into compliance!
by Annette Huenke | Jan 25, 2021 | General
Huge breaking news! Jefferson Healthcare’s response to a Public Records Request just revealed jaw-dropping information: It is using a PCR assay with an absurdly high cycle threshold of 45, calling into question ALL of Jefferson County’s reported COVID-19 cases!
To understand what this means and why it’s so important requires a deep dive into the world of PCR testing. Establishment media outlets don’t go there. Instead they rush to trumpet the following sort of claims without investigating details:
“Port Townsend woman tests positive for COVID-19.” That’s the headline of a January 21, 2021 article in The Port Townsend Leader. “The number of confirmed COVID-19 cases in Jefferson County,” the Leader reports, “rose to 274 Wednesday as Jefferson County public health officials reported a Port Townsend woman in her 40’s had tested positive for the disease.”
What exactly does it mean if someone tests positive? What do these numbers really tell us?
As early as last spring, several concerned Jefferson County citizens began warning the county commissioners and Board of Health that authoritative research was proving PCR test results to be plagued with a high percentage of false positives. That warning was echoed by Canadian pathologist Dr. Roger Hodkinson [linked here] whose company sells a COVID-19 PCR test. Oxford University scientist Dr. Tom Jefferson sounded the alarm again in a Daily Mail article, as did a review by the University of Oxford’s Centre for Evidence-Based Medicine. Just last week, these concerns were affirmed in new guidance from the World Health Organization.
As Dr. Tom Jefferson explains, these PCR tests “are telling people they have Covid-19 when they do not. In some cases, for example, viral RNA might be present in such very low quantities that an individual is not at all infectious and poses zero danger. In other cases, the swabs might pick up RNA which is so old it is completely dead, as people continue shedding material from the virus up to 80 days after the initial infection.”
Reverse transcription polymerase chain reaction (RT-PCR) is a laboratory technique used to detect the presence of ribonucleic acid (RNA) purportedly unique to SARS-CoV-2. It does this through amplification of molecular material in what are called cycles, with the top numerical end of those cycles known as the threshold (Ct).
In an August 29, 2020 article in the New York Times titled “Your Coronavirus Test is Positive. Maybe it shouldn’t be,” the author writes “Most tests set the limit at 40, a few at 37. This means that you are positive for the coronavirus if the test process required up to 40 cycles, or 37, to detect the virus.” According to Dr. Michael Mina, an epidemiologist at Harvard’s T.H. Chan School of Public Health, tests with thresholds so high may detect not just live virus but also genetic fragments, leftovers from infection that pose no particular risk— akin to finding a hair in a room long after a person has left. “Any test with a cycle threshold above 35 is too sensitive,” agreed Juliet Morrison, a virologist at the University of California, Riverside. “I’m shocked that people would think 40 could represent a positive,” she said. A more reasonable cutoff would be 30 to 35, she added. Dr. Mina says he would “set the figure at 30, or even less.”
The article continues: “The C.D.C.’s own calculations suggest that it is extremely difficult to detect any live virus in a sample above a threshold of 33 cycles.”
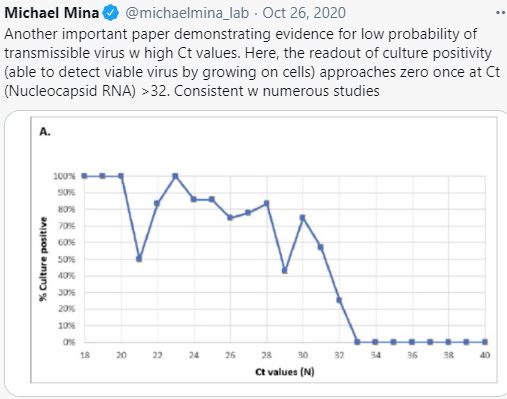
Dr. Mina posted this chart on October 26, 2020, demonstrating evidence for low probability of transmissible virus with high Ct values, in other words, how running more than 32 cycles can produce a practically meaningless positive test result. He wrote, “The readout of future positivity (able to detect viable virus by growing on cells) approaches zero once at Ct (nucleocapsid RNA) >32. Consistent with numerous studies.”
In a July 16, 2020 interview on This Week in Virology, Dr. Anthony Fauci said, “If you get a cycle threshold of 35 or more…the chances of it being replication competent are minuscule. You almost never can culture a virus from a 37 threshold cycle. So I think if someone does come in with a 37, 38, even 36, ya gotta say, ya know, just dead nucleotides. Period.”
Last November a Portuguese court ruled that the PCR test was too unreliable to use it in justifying quarantines. The ruling relied upon a number of scientific studies, including one by Jaafar et. al, which found that, “when running PCR tests with 35 cycles or more, the accuracy dropped to 3%, meaning up to 97% of positive results could be false positives.” The ruling concluded that, based on the current state of science examined by the court, any PCR test using over 25 cycles is totally unreliable.
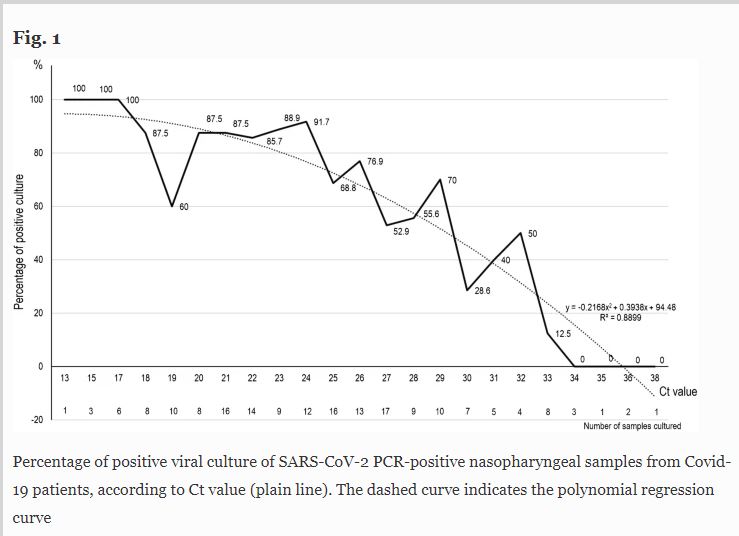
Yet another reputable study, by La Scola, et. al, published in the European Journal of Clinical Microbiology and Infectious Diseases, similarly found that the reliability of these tests drops significantly at 24-25 cycles, and, like the Mina graph, flat-lines at 34 cycles. “[P]atients,” according to the study, “with Ct values above 34 do not excrete infectious viral particles.”
Jefferson County’s Health Officer, Dr. Thomas Locke, has been tight-lipped about the cycle thresholds behind the positive COVID cases his department has been reporting. That is why I submitted my public records request to Jefferson Healthcare to uncover their protocols. They disclosed to me that they are using a PCR assay with a 45-cycle threshold, well beyond the outer limits of reliability.
Someone testing positive in Jefferson County using a 45-cycle threshold that has near-zero accuracy may be labeled a “case” by our health department. A healthy person with no respiratory illness whatsoever can be called a COVID “case”. If a person seeks medical care at Jefferson Healthcare for a stroke or heart attack and then tests positive with this unreliable test, they may be erroneously put in the hospital’s COVID ward and added to county “case” numbers.
The assay being used in this county has been designed to terminate the cycling automatically if the viral load is high. If it truly functions as intended, one can reasonably assume that not all 274 “cases” cycled up to the 45 Ct. But we have no idea how many cycles have been repeated on each “case” for the positive test results.
What’s needed by our Public Health Officer is to report the cycle count for every positive case so it can be individually evaluated, as the Florida Health Department has mandated. Then an overall false positive rate for the county could be more reliably estimated.
“Case” numbers are being used to justify authoritarian policies here and around the globe. This is institutional fraud on a scale without precedent. These numbers are being used to terrorize the public into viewing one another as an imminent, potentially deadly, threat. Our local businesses are being crushed, children’s education throttled, our social engagement eviscerated and futures of young families jeopardized for this colossal mirage of “cases.” There is a very real possibility that the young generation will never again feel safe in the presence of strangers.
Public health bureaucrats have effectively been given police powers. Censorship has been weaponized by a technocratic elite to the degree that anyone who challenges the official narrative can expect a backlash of demonization, deplatforming and purging from social media and other public forums. Our own local print media is censoring letters to the editor, even paid advertisements that contain factual data from incontestable sources, if the information differs from that promoted by local authorities. The local radio station is regurgitating those same authorities’ pronouncements as though their veracity is holy and above examination.
Claims of escalating numbers of “cases” are central to maintaining the fear locomotion that demands masking, distancing, quarantines, lockdowns and now, a population-wide clinical trial of an experimental vaccine.
It is past time to hit the pause button, to stop and ask the question— what is going on here?
by Stephen Schumacher | Jan 14, 2021 | General
“Second person in Jefferson County dies from COVID-19” trumpets the January 13 Leader’s front-page headline.
https://www.ptleader.com/stories/update-second-person-in-jefferson-county-dies-from-covid-19,73202
She was “an 80-year-old woman who was being treated in a Seattle-area hospital” since “late October for surgery unrelated to the coronavirus. Following the surgery, she developed complications which mandated additional hospitalization.
“In early December she became infected with COVID-19 as part of a hospital wide outbreak” and “passed away Dec.26.” Her death was not immediately considered to have been caused by COVID, according to Dr. Tom Locke, Jefferson County’s Health Officer. “[S]tate officials were brought in to investigate the death and determine whether her death should be classified as COVID-related or having to do with one of her multiple previously existing medical conditions.”
This second Jeffco death blamed on COVID-19 is even more dubious than the first, a hospice patient in her 90’s. In additional to multiple comorbidities, this 80-year-old woman, suffering what appear to have been extremely serious complications from surgery, had not been near Jefferson County for 2 months when she contracted COVID-19. All events surrounding her death took place in the Seattle area.
Below is a letter I wrote questioning Jeffco’s earlier death, which the Leader and Peninsula Daily News declined to publish. Its closing line appears to be still accurate: “Based on information reported to date, Jefferson County still seems to have no deaths from COVID-19.”
Dear Editor,
I respectfully question the basis on which “Jefferson County just recorded its first death from COVID-19 last week.”
The decedent was “in her 90s and was chronically ill and had been receiving hospice care,” meaning she was already on the verge of death with no hope of cure. She may have died WITH the virus, but I doubt she died FROM the virus.
This is a classic example of how shifting standards and incentives have inflated COVID-19 death totals. Coronavirus illnesses like colds didn’t count as the cause of death for hospice patients in years gone by.
But nowadays, “if you were in hospice and had already been given a few weeks to live, and then you also were found to have COVID, that would be counted as a COVID death… anyone who passes away after testing positive for the virus is included in that category,” per Illinois’ Health Director.
Hence our county’s “first death from COVID-19” would be “included in that category…after testing positive” whether or not she had any COVID symptoms hastening her already-imminent departure.
Note how this miscounts (often false) positive PCR tests for the SARS-CoV-2 virus as if they were symptomatic cases of the disease COVID-19, further inflating “case” and death statistics. Like HIV and AIDS, the virus and the disease are different concepts and should
not be lumped together.
Based on information reported to date, Jefferson County still seems to have no deaths from COVID-19.
— source links —
https://www.ptleader.com/stories/first-death-from-covid-19-reported-in-jefferson-county,72373
https://www.ptleader.com/stories/covid-19-death-linked-to-senior-care-facility,72394
https://www.mayoclinic.org/healthy-lifestyle/end-of-life/in-depth/hospice-care/art-20048050
https://week.com/2020/04/20/idph-director-explains-how-covid-deaths-are-classified/
https://www.nytimes.com/2020/08/29/health/coronavirus-testing.html
https://twitter.com/kylamb8/status/1332428342251950087
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it
by Jim Scarantino | Jan 12, 2021 | General
Port Townsend Free Press is going quiet for several months. The editor, Jim Scarantino, as in 2019, has to get to work on business responsibilities here and on the East Coast. Due to the COVID lockdowns, there’s a significant backlog needing attention. Plus, he’s going to to be doing a little traveling and enjoying those states within driving distance where one can dine and drink inside a bar and restaurant.
Thanks to everyone who contributed to our humble effort at citizen journalism during 2020: Brett Nunn, Craig Durgan, Gabrielle Guthrie, Gene Farr, Z Cerveney, Steve Schumacher, T.J, Kalas and our “Concerned Citizen of Port Townsend,” whose incisive commentaries we agreed to publish anonymously because she feared retaliation. Your articles were widely read. You made a real contribution to the dialogue in Jefferson County.
And thanks enormously to our readers–those who openly followed our work by commenting, sharing our stuff, or “liking” or “following” on Facebook–and the many more who regularly read our work but don’t want others in Port Townsend to know. Thanks for letting us know you’re out there. Our numbers soared this past year, and it was all because of all of you.
The lawsuit Jim Scarantino filed against Jefferson County for the way it censors and stifles speech in its on-line public forum, its official Facebook page, is proceeding, regardless of other commitments.
See you in a bit. Thanks for your understanding.