by Jim Scarantino | Feb 25, 2021 | General
Banned for encouraging people to never forget 9/11.
Sanctioned for mentioning Jefferson County’s terrible meth problem, chronic unemployment, shrinking job base and high poverty rate.
That’s what I’ve learned about how Jefferson County operates the public forum of it’s official Facebook page. Thanks to the people who sued President Trump and won when he blocked them from his Twitter feed, the law is clear that the First Amendment governs the actions of public officials in how they manage their official social media forums. They cannot engage in content-based discrimination. They cannot retaliate or punish. They cannot suppress speech that does not fall into one of the very limited exceptions of the First Amendment.
Encouraging people to remember the terrorist attacks, deaths and heroism of 9/11….definitely protected speech. Speaking out on our county’s drug and economic problems….definitely protected speech. But it is for expressing those opinions that I was sanctioned by whichever public official made those decisions.
So I sued Jefferson County in federal court for these First Amendment violations.
Thanks to the answer filed by Jefferson County in the case, I saw where I had incorrectly reconstructed what I believed happened on 9/10/20, where I thought this story started. I had believed that a comment about COVID issues had been deleted. I was wrong. The county has the activity log that shows they “hid” my comment that linked to a video about 9/11. That video is a gut-wrenching thing to watch, because what happened on that day was and is forever a nightmare to anyone with an ounce of love for life, liberty and this nation of ours.
Watch it for yourself: https://www.prageru.com/video/9-11-we-must-never-forget/
Why would the Jefferson County government not want people remembering 9/11? What was so objectionable about that video that I was later banned from participating in discussions on this public forum?
What I learned is that the county will make invisible comments it does not want other people to see. The author may see the comment and does not know that it has been made invisible to most everyone else. You could be seeing a comment from someone that has been made invisible to others because you happened to have “friended” that person (though you may not actually know them). You will have no idea that you could be alone in receiving what that person has to say about matters of public concern and county business.
The county says they made my 9/11 video link invisible because it was “off topic.” I am not aware that “off topic” is a recognized ground for government to censor or sanction speech. I know of no case at this time holding that “off topic” is an exception to the First Amendment. But “off topic” is their excuse.
I posted the video about 9/11 on 9/10 for good reason. The county’s Facebook page has published proclamations on other things, such as Earth Day. It had made no mention whatsoever of any commemoration of 9/11. My comment was intended to correct that omission. It was a protest of the county’s failure to honor that day and those who died and an attempt to bring attention to that failure. Protesting and bringing attention to a government’s failure is pure political speech that cannot be censored. The county saying it was “off topic” (it wasn’t) doesn’t outrank the First Amendment. The City of Port Townsend at the time was embroiled in a growing controversy because it had cancelled the annual ringing of the old fire bell at the hour the first plane hit the Twin Towers. The county was not indicating it would honor that day. It was silent about 9/11. So I posted that “Never Forget 9/11” video. This is pure political speech protected by the First Amendment.
The next day, 9/11, came and went without any mention by the county of the events of that day in 2001. Courthouse bells rang, but without any explanation by the county.
Sometime after that I was banned from participating in the public forum the county created with its official Facebook page that allows comments (except those it disagrees with). I could not comment. I could not even “like” or “dislike” a pronouncement or news development published by the county.
I had received no notice that I had been sanctioned or why. That is something else I’ve discovered since I filed suit: the county sanctions people–deleting or “hiding” their comments, banning them from commenting–without any notice or explanation. As I mentioned, if you receive the sanction of your speech being “hidden” you have no idea that has happened. You have to sit down with someone who is not a Facebook friend and ask them if they can see on their computer what you wrote. If they cannot, then you just learned you have received the official sanction of having your speech censored.
There is no appeal process. You can sue, though you shouldn’t have to.
After my lawsuit was served on the county, they seem to have lifted (without notice to me) the sanction that prevented me from expressing opinions and sharing information to others viewing their Facebook public forum.
Then they again sanctioned me without notice, without explanation. I discovered that a comment I made in January 2021 about the county’s terrible meth problem, chronic poverty, shrinking job base and severe poverty resulted in the county sanction of making the comment invisible. The sanction was curious, because I was responding to a comment by another person about some of the same problems, particularly the drug problem right now at the County Fairgrounds where a young woman, a meth user, was found dead, lying face down on the ground in the open where in happier times children have played and people have enjoyed rides and 4-H animal exhibits.
I don’t know if my comment about our terrible meth problem was made invisible by county officials before or after the campground manager came across this poor woman’s stone-cold body and called police.
The county says it prohibits profanity, but now that I’ve examined the entire history of comments I see an F-bomb and other profanity. The county says it prohibits promotion of business and political candidates, but I’ve found examples of that. The county says it prohibits insults and personal attacks, but I’ve found plenty of those. The county says it prohibits comments that embed images from external sources or that contain copyrighted material. I’ve also found plenty of examples where they don’t enforce that rule, either. But the county sure is good at prohibiting my speech when it disagrees with the narrative they want enforced in that public forum.
I intend to amend my complaint to include these facts and others I’ve learned since our initial pleading. There will be a bit of a delay. My attorney suffered a health crisis requiring emergency surgery. The county’s attorney has graciously agreed to push things back 90 days. I also still hope we can settle this.
Given the pesky First Amendment, running an official government social media site is fraught with problems. Every decision the county makes about its Facebook page is state action triggering First Amendment review. As I’ve learned, it also triggers rights of due process. I hope my attorney and I in cooperation with the county can find a solution that cures the currently unconstitutional and illegal manner in which the county is managing this public forum.
A curious thing occurred recently. In response to publication of a proclamation by the Board of County Commissioners in January about the Port Townsend Women’s March, I posted in a comment the same “Never Forget 9/11” video that got me banned after I posted it on 9/10/20. Nothing happened. The comment was not made invisible and my First Amendment rights to participate in the public forum were not taken from me.
Like I said, one shouldn’t have to file a federal lawsuit to prevent the government from censoring his political speech. But apparently going to court does improve how a citizen gets treated.
by Jim Scarantino | Feb 23, 2021 | General
Annette Huenke through a public records request discovered that Jefferson Healthcare’s Covid testing protocols may run samples through so many amplifications that the result may be a false positive or otherwise meaningless. We were pleased to publish the results of her inquiries, “Is Jefferson County Health Department Overstating COVID Numbers?”
Huenke has continued to try to nail down the scientific data behind claims made by the Jefferson County Health Department to determine if they are accurate and should be relied upon by policy makers and citizens. Recently, claims about the benefits of double-masking have been asserted. Huenke wanted to know what there was in the way of scientific studies and data to back those claims up. Following is her exchange on the subject with Dr. Thomas Locke, Jefferson County Health Officer.
You may ask, Where does Ms. Huenke get off investigating statements by Dr. Locke? How dare she question “the science”? Isn’t Port Townsend Free Press contributing to unscientific “pandemic denialism” by giving her a forum? After all, she is not “an expert.” Are we not just spreading “disinformation”?
“Science is the belief in the ignorance of experts.”
Those are the sage words of Nobel-winning physicist and philosopher of science, Richard Feynman. He was referring to “science” which determines policies through the weight of expert and political consensus. This is the stuff we get on the evening news and what is being forced upon us by Facebook’s, Twitter’s and YouTube’s–and our local newspapers’–censorship of anything that might cast doubt upon the establishment consensus, even if those doubts are raised by people who happen to be scientists and rigorously employ the scientific method in their research.
Feynman said, “Learn from science that you must doubt the experts.” We return to Feynman at the end of this article, and link one of his famous lectures on the scientific method.
Here follow Ms. Huenke’s efforts to get the empirical science on the political science of double-masking. Much more comes to light than the simple answers she sought.
From: Annette Huenke, 2/8/21, to Jefferson County Board of Health and Dr. Locke
Subject: re: this morning’s BOCC meeting.
Good afternoon, all. This morning Dr. Locke said that “there is a lot of evidence” to support double-masking.
Kindly provide that evidence in a reply to this email at your earliest convenience. Thank you.
Annette Huenke
_______________________________________________
Dr. Locke’s reply, 2/8/21:
The rationale for double masking (spun polypropylene inner mask, two layer cotton outer) is based on an enhanced mechanical filtration effect (extra layers) and an electrostatic charge being generated (triboelectric effect) by dissimilar fabrics. CDC is conducting comparative studies of masking efficacy but this will likely be confined to filtration measures. “Hard data” (epidemiological studies demonstrating decreased transmission and/or acquisition of infection) are much more difficult and raise ethical concerns (re: control groups use of substandard or no PPE). And no amount of data will convince people who are consumed by pandemic denialism and wish to rationalize their pseudoscientific, sociopathic beliefs.
Tom Locke, MD, MPH
Jefferson County Health Officer
Huenke’s 2/14 response to Locke’s 2/8 letter:
Ad hominem attacks are unbecoming a man in your position, Dr. Locke, and says a lot more about you than it does about those you are eager to insult. Pathologizing dissent is not a new tactic for marginalizing unwelcome voices. So-called ‘witches’ were similarly outed in their communities and burned at the stake for such digressions. The strategy was perhaps perfected by the Soviets in the mid-twentieth century, deployed against anyone who deviated from the official narrative.
For ten months now a handful of concerned citizen researchers have been highlighting bona fide studies from reputable sources to broaden the perspective of local policy makers. Those sources include the CDC, WHO and top scientists and universities around the globe.
Last Monday you stated publicly that “there is a lot of evidence” to support double-masking. ‘A lot of evidence’ turns out to be a NIH ‘commentary’ that purports to “summarize the evidence on face masks for Covid-19 from both the infectious diseases and physical science viewpoints.” Similar to the ‘evidence review’ you provided the board on May 21st last year, this one manages to summarize evidence that supports the goals of its funders while ignoring the plethora of research that does not. It is a text book example of cherry-picking.
“A lot of evidence” for double-masking is actually several small mechanistic experiments conducted with manikins. Manikins don’t breathe. Employing the tired “it would be unethical” trope, in this case to deny proper PPE to a control group, rings hollow when we know full well that there is a sizable portion of the population that can’t or won’t wear masks.
In an
AFT Fireside Chat on January 28th, just over two weeks ago, Anthony Fauci said “There’s no evidence that indicates that that [2 masks] is going to make a difference. And that is why the CDC has not changed their recommendation.” He’d advised double-masking shortly before that, surely aware that this ‘commentary’ was soon to be released.
You have steadfastly rejected the research we’ve supplied that demonstrates known harms from masking. You haven’t expressed real concern about improper use and care of the masks you relentlessly promote. Sadly, you’re now encouraging people to further reduce their oxygen supply and increase their own carbon dioxide intake.
You and your colleagues do not have a corner on valid science. You are not all-knowing, all-seeing, infallible. Thousands of experts with credentials that exceed yours, John Wiesman’s and Anthony Fauci’s disagree with you. That they are being censored and you are not is the reveal. Censorship is employed by authorities to conceal the truth.
I offer you a table turned — “no amount of data will convince people who are consumed by pandemic” propaganda “and wish to rationalize their pseudoscientific, sociopathic beliefs.”
Annette Huenke
___________________________
Huenke’s comment for 2/17 Board of County Commissioners meeting:
At last week’s BOCC meeting, Dr. Locke said that “there is a lot of evidence” to support double-masking. I wrote to ask for that evidence. I received a pdf of a 4-page paper and a brief reply that ended with “no amount of data will convince people who are consumed by pandemic denialism and wish to rationalize their pseudoscientific, sociopathic beliefs.”
For ten months now a handful of concerned citizen researchers have been highlighting bona fide studies from reputable sources to broaden the perspective of local policy makers. Those sources include the CDC, WHO and top universities and scientists around the globe. Are those premiere virologists, pathologists and epidemiologists pseudoscientists because they’ve arrived at different conclusions than Dr. Locke about the crisis that is consuming us? Are we sociopaths because we consider the research and opinions of those experts?
What Dr. Locke called “a lot of evidence” for double-masking is actually several small mechanistic experiments conducted with manikins, reported in a NIH ‘commentary’ that summarizes studies which clearly support the goals of its funders while ignoring the plethora of research that does not. It was not peer reviewed. It is data-deficient.
During a fireside chat on January 28th, Anthony Fauci said “There’s no data that indicates that that [2 masks] is going to make a difference. And that is why the CDC has not changed their recommendation.” He’d advised double-masking shortly before that, surely aware that this NIH paper was in its final stages.
In a recent interview, Dr. Michael Osterholm, a top health adviser to President Biden, warned that double-masking could be counterproductive and harmful. “If you put more of it on, all it does is it impedes the air coming through and it makes it blow in and out along the sides. The fit becomes even less effective,” he said. “Double masking could be a detriment to your protection.”
Legitimate research we’ve supplied that report known harms from masking has been categorically rejected. There has been scant attention paid to the near-universal improper use and care of masks, which has been proven to increase risk of infection. And now, based on experiments with manikins, we’re being told to wear two masks, which will further reduce our oxygen supply and increase our own carbon dioxide intake.
A true cost/benefit analysis of these extreme masking policies has not yet been conducted. Neither has the rigorous scientific research required to support them.
Annette Huenke
___________________________
Dr. Locke’s reply to Huenke’s BOCC comment, 2/17:
Ms. Huenke,
All science-based information has elements of uncertainty and is subject to challenge and, hopefully, increasing reliability. This is how the scientific method works. I agree it is wrong to pathologize dissent or to marginalize unwelcome voices. Just as there is science, which seeks to establish the true nature of things, there is also pseudoscience, which perverts that process by selectively citing supporting information while ignoring or distorting non-supporting information. It can be difficult for the general public to distinguish between the two. The COVID-19 pandemic is the worst public health crisis that the U.S. has faced in the past 100 years. It’s management has been seriously compromised by those who embraced and promoted “alternative facts” to support their views that non-pharmacological mitigations like masking, distancing, and restricted gatherings are a fundamental violation of human rights. The Great Barrington Declaration and the ongoing pseudoscientific opposition to mask use are examples of this phenomenon and pit individual liberty against public health. The CDC reliably estimates that 59% of SARS-CoV-2 infections are transmitted by asymptomatic cases (35% presymptomatic, 24% never symptomatic). Universal masking is the only viable strategy to interrupt this transmission pathway and has a growing evidentiary base. Attached are some additional links from recent CDC publications. Based on what we currently know, the refusal to wear masks in public settings at times of high COVID-19 prevalence is truly sociopathic — antisocial behavior characterized by the willful disregard of the welfare of others. It is also illegal. I do not think it is not too much to ask to prevent a potentially lethal infection in someone else.
I am sorry that you took personal offense at my statement that “no amount of data will convince people who are consumed by pandemic denialism and wish to rationalize their pseudoscientific, sociopathic beliefs.” In this statement I am referring to the well recognized phenomena of the “unpersuadable” (The Unpersuadables: Adventures with the Enemies of Science by Will Storr (goodreads.com)<https://www.goodreads.com/book/show/18114379-the-unpersuadables>), those who reject scientific information because it is in conflict with their fundamental, non-rational worldview. No amount of information will change the mind of someone who is unpersuadable. This worldview drives the “anti-vaxxer” movement and has been dramatically amplified by the ubiquity of social media and the ability of people to curate their own reality by selective exposure to only those facts that support their worldview. I am always happy to consider alternative views but have come to recognize the futility of arguing with those who only seek the confirmation of their own beliefs. My prime responsibility as the county health officer is to control the spread of SARS-CoV-2 in this community and to reduce morbidity and mortality to the greatest extent feasible. This battle is very real and we deal with individuals and families who lives are profoundly disrupted by this pandemic every day. As a nation we have paid a terrible price for pandemic denialism — a very high death rate (currently at 485,000) and a case rate (27 million) far in excess of what a country with our resources and technology could have achieved. These are not just harmless differences of opinion, they have real world consequences.
You cite Dr. Anthony Fauci, a distinguished infectious disease specialist, but you do so out of context. In other public statements he has supported masking, including improved mask design and the benefits of “double masking”. Double masking is not a panacea for the problem of SARS-CoV-2 transmission, but is one more option. The takeaway from the CDC information and similar research to date is that people should use high quality masks and use them in situations where asymptomatic transmission can occur. If we fail, once again, to make reasonable personal sacrifices for the common good, it is likely that SARS-CoV-2 variants will spread faster than vaccination efforts can suppress them, necessitating renewed school and business closures.
While your comments to the Boards of Health and County Commissioners are always welcome, I am unable to continue to respond personally to your statements due to time limitations. I regard the CDC as an authoritative source of information, especially under the leadership of the Biden administration and refer you to their various websites and publications for the latest research on the topics you are interested in.
Sincerely,
Tom Locke, MD, MPH
Jefferson County Health Officer
“Science says….”
The Great Barrington Declaration that Dr. Locke dismisses as “unscientific” and “pandemic denialism” is a declaration of concern about Covid policies signed by infectious disease epidemiologists and public health scientists from around the world. It advocates a “focused protection” approach to those most at risk and seeks to avoid the many serious problems caused by general Covid lockdowns. Dr. Locke’s glib dismissal of this challenge to Covid policies–challenges based on these individuals’ work and learning in their fields of scientific and medical expertise–brings us back to Feynman’s definition of “science” and why we are pleased to give people like Ms. Huenke (and Dr. Rob Rennebohm, Stephen Schumacher and Ana Wolpin) a forum for their questions about prevailing Covid policies and liturgies.
In closing, here’s more from Feynman on why science is “belief in the ignorance of experts”:
When someone says, “Science teaches such and such”, he is using the word incorrectly. Science doesn’t teach anything; experience teaches it. If they say to you, “Science has shown such and such”, you might ask, “How does science show it? How did the scientists find out? How? What? Where?” It should not be “science has shown” but “this experiment, this effect, has shown”. And you have as much right as anyone else, upon hearing about the experiments–but be patient and listen to all the evidence–to judge whether a sensible conclusion has been arrived at…The experts who are leading you may be wrong…I think we live in an unscientific age in which almost all the buffeting of communications and television-words, books, and so on-are unscientific. As a result, there is a considerable amount of intellectual tyranny in the name of science…Science alone of all the subjects contains within itself the lesson of the danger of belief in the infallibility of the greatest teachers of the preceding generation.
Richard Feynman on Scientific Method (1964) – YouTube
Related: CDC on Maximizing Fit for Cloth and Medical Procedure Masks
CDC: The Science of Masking to Control COVID-19
[Ms. Huenke’s 2/14 response to Dr. Locke’s 2/8 letter was omitted inadvertently from the initial publication of this article]
by Ana Wolpin | Feb 20, 2021 | General
“Locke…is concerned about a Jefferson County group that may be spreading misinformation concerning the accuracy of the tests, claiming incorrectly that up to 90 percent of COVID-19 tests provide false positives.” [Peninsula Daily News, 2/7/21]
“Public naysaying on the spread of COVID-19 continued at Monday’s meeting of the board of county commissioners, with the public comment period being marked by more claims of false positive COVID-19 tests by some Jefferson County residents… ‘That kind of denialism is becoming more dangerous,’ Locke said.” [The Port Townsend & Jefferson County Leader, 2/3/21]
Who are these citizens being called dangerous by Jefferson County’s Health Officer, Dr. Thomas Locke? They are concerned citizens being censored by all media on the peninsula except the Port Townsend Free Press.
I am among them.
Dangerous Misinformation?
Over the past year, a group of local researchers has diligently examined data and analyzed information driving the global policies now devastating our world. Independent of our efforts, Stephen Schumacher was also deeply researching, coming to similar conclusions that much of the fear narrative being broadcast didn’t hold up to scrutiny.
In July 2020, Schumacher submitted a letter to the Port Townsend Leader citing statistics related to COVID-19 (Covid) lockdowns. His letter was withheld from publication for nearly a month, but eventually ran.
The following month, the Leader flatly refused to print his next letter. Unable to participate in the community opinion forum which “welcome[s] letters from our readers,” Schumacher then paid $500 to purchase ad space to share his information. A second ad, at the end of August, costing $550, warned about problems with the now-infamous discredited models Dr. Locke was citing to justify lockdowns. This was followed by two more ads regarding lockdowns in September and October.
In November, the Leader took censorship to the next level. After first accepting a paid ad about concerns over PCR tests, the publisher emailed Schumacher to inform him that they would not be running it. His ad featured a graph from a Harvard epidemiologist, and cited the Journal of the American Medical Association, the CDC, and other mainstream sources. In an email exchange asking why he was being censored, the publisher wrote, “We need to make decisions based on the best interest of our business.”
Was the payment Schumacher offered to exercise his right for freedom of expression insufficient when weighed against the newspaper’s role as a propaganda arm of Dr. Locke?
Schumacher took his rejected ad to the Peninsula Daily News. The PDN first agreed to accept his $530, then balked. The ad ultimately ran on Nov. 22. Several weeks later he attempted to buy ad space there a second time, but was told the publisher had rejected it. “When I asked if there was something specific I could have tweaked to make the ad acceptable, the answer was negative,” he said. “The content was verboten.”
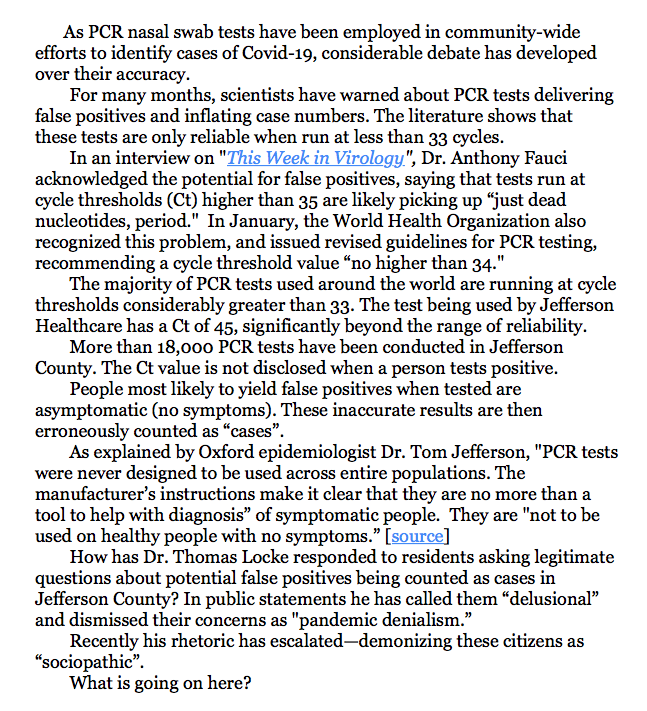
PCR tests come into focus
While local censorship was ramping up, many scientists were expressing concerns that the PCR tests, responsible for exploding “case” counts and continued lockdowns, were not reliable. In some experts’ words, they are “not fit for purpose.” Most of this information was also being suppressed.
But on August 29, 2020, the New York Times published the story, “Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be.” It quoted Harvard epidemiologist Dr. Michael Mina: “from 85 to 90 percent of people who tested positive in July with a cycle threshold [Ct] of 40 would have been deemed negative if the threshold were 30 cycles.”
Evidence mounted that cycle thresholds are critical, confirming the New York Times story.
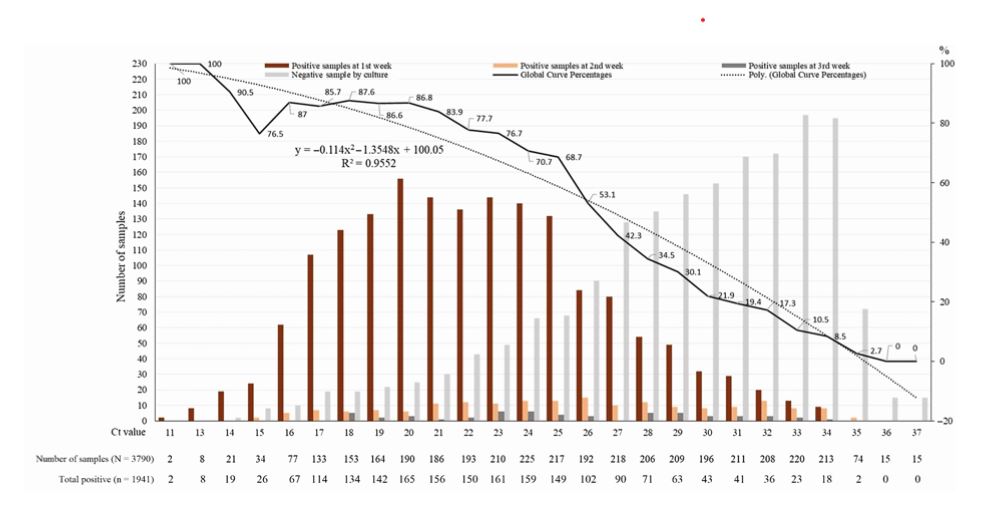
In a September article in Clinical Infectious Diseases, a French team looked at more than 100 studies on PCR tests. All studies found that above 30 cycles “patients could not be contagious as the virus is not detected in culture above this value.” They then performed 3790 of their own tests, reporting similar findings—of the samples that tested positive after 35 PCR cycles, 97% were negative upon viral culture. And of samples testing positive after 37 or more cycles, 100% were culture negative.
The lack of PCR reliability was reinforced in November by an international group of experts who formally challenged these tests as a valid diagnostic tool for identifying Covid cases. In their extensive report—“External peer review of the RTPCR test to detect SARS-CoV-2 reveals 10 major scientific flaws at the molecular and methodological level: consequences for false positive results”—the authors contend that serious defects in the test have “led to worldwide misdiagnosis of infections.” They conclude that the test is “completely unreliable” and “unsuitable as a specific diagnostic tool to identify the SARS-CoV-2 virus.”
In December, an Italian team documented that when the Covid PCR test is positive only at a high Ct value, the incidence of false positivity is at least 70%. Their article in the Journal of Clinical Virology warns that the detection of viral RNA at a high cycle threshold “needs to be interpreted with caution.”
Revised guidelines from the World Health Organization followed in January. All parties agree that beyond 30-35 cycles, the PCR test cannot reliably provide accurate identification of a Covid case, calling into question case figures worldwide.
Is this incontestable global consensus—that at high cycle thresholds PCR tests yield mostly false positives—the “misinformation” that Locke speaks of in the PDN quote above?
As revealed by Annette Huenke in her Port Townsend Free Press article, “Is Jefferson County Health Department Overstating COVID Case Numbers?,” the cycle threshold of the PCR test being used in Jefferson County is not 30 or 35 or even 40. It is 45. No scientist disputes that with a positive result at 45 Ct, the chance of infection is zero.
Our test results do not report the cycle count; they merely declare a binary positive or negative. Without the Ct information there is no way to judge viral load, or if the test simply picked up dead viral debris; if the person is contagious, or if the result is a false positive.
Locke has yet to disprove any of this information.
Censorship and Demonization: the New Normal
For several months I have been among the citizens writing to our county commissioners about this concern. In response, the commissioners repeatedly defer to their expert, Locke. He waves off any responsibility, passing the buck to state authorities—not my problem—while insulting the citizens bringing these issues to light.
Locke’s attacks have grown increasingly shrill and aggressive towards residents challenging his pronouncements. In a response to a brief request from Annette Huenke asking for data he had referenced in a weekly report broadcast on KPTZ, Locke concluded his email with:
“And no amount of data will convince people who are consumed by pandemic denialism and wish to rationalize their pseudoscientific, sociopathic beliefs.”
In addition to the “pandemic denialism” pejorative he has been using for months, the county’s Public Health Director is now calling citizens who ask relevant, important questions “sociopaths”. It is no wonder that increasing divisiveness is pervading our community.
Our voice is censored by all local media except this online publication. When some of us raised the issue with our county commissioners of free speech being denied by the mainstream press, Commissioner Greg Brotherton rationalized that it was important to have “a unified approach” in messaging the public. That is a euphemism for “official propaganda only.”
The newspapers not only refuse to investigate valid citizen concerns, they allow no right of rebuttal to Locke’s messaging and name-calling.
On February 10, I submitted this letter to the Leader:
To date, the Leader has not run my letter.
12/23/20 protest outside office of PT Leader
Nor has a letter about PCR tests from Dr. Robert Rennebohm been published, submitted a week prior to mine. An MD who has extensively researched Covid issues, Rennebohm stresses the importance of disclosing Ct values in reporting new Covid cases, underscoring the need for and responsibility of public health departments to change course:
“Medically, morally, and ethically—individuals with positive PCR tests, as well as physicians, epidemiologists, public policy makers, and the public—deserve to know, and need to know, the Ct value at which a SARS-CoV-2 PCR test is positive. Without Ct information, interpretation of the number of “new COVID cases,” “new COVID hospitalizations” and “new COVID deaths” is severely compromised, as is public policy and the care of individual patients.”
Rennebohm’s detailed explanation of Ct values can be read in the Port Townsend Free Press article, The Importance Of Knowing The Ct Value At Which SARS-CoV-2 PCR Tests Are Positive.
But not even a credentialed physician, one who I daresay has greater understanding of PCR’s uses and limitations than Locke, is permitted to offer a professional perspective in the Leader if it diverges from Jefferson County’s Public Health Director. Rather than requesting interviews or promoting healthy debate on an issue that is profoundly impacting every one of us, there is only the silencing of any viewpoint that does not support the official narrative. A “unified approach.”
Valid, scientifically confirmed concerns should generate robust public discussion in our community. Instead, county residents are deluged with one-sided information that is often inaccurate and falls significantly short of adequately educating the public. Area newspapers, the local radio station, and other media provide a bully pulpit for Locke to disseminate what many scientists around the world would argue is misinformation.
Reporting all sides of a story is the fundamental purpose of journalism, the recognition that a fully informed citizenry is the foundation of democracy. That has been suspended in our New Normal. Allowing diverse voices to engage in civil discourse is deemed dangerous.
Cycle threshold values are only a small part of the PCR story, the one that has gotten the most attention. Equally critical is the clear instruction—in accordance with the PCR test’s authorized labeling—that its use should be limited to symptomatic individuals… not inflicted across entire communities of people who, for the most part, are not sick.
On January 4, the Food and Drug Administration released “Risk of False Results with the Curative SARS-Cov-2 Test for COVID-19: FDA Safety Communication.” The FDA’s direction to healthcare providers, patients and caregivers is that PCR test use should be “limited to individuals within 14 days of COVID-19 symptoms onset.” Use on asymptomatic people or outside the two-week window was likely to produce false results, or at least inadequately interpretable results.
The story in Jefferson County
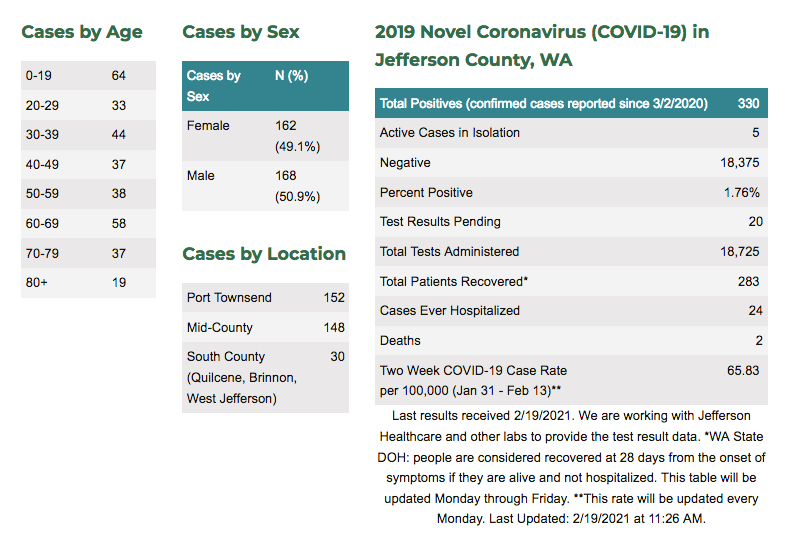
Of more than 18,700 tests administered in Jefferson County since March 3, 2020, over 300 cases have been identified as “positive” to date.
This includes symptomatic people—those with Covid symptoms like fever, body aches, and sore throat—who may have been tested within the 14-days-of-onset window.
It also includes people tested who had NO Covid symptoms—those who are in facilities or jobs that require testing; who go to the hospital for unrelated elective procedures; who are admitted to the ER after a heart attack, stroke, or accident; and those who ask to be tested out of fear, or curiosity—some of them getting multiple tests. None of these meet the criteria of showing symptoms in a 14-day window. Most of those tests are inadvisable and prone to false positives.
The only people with positive tests who can arguably be called legitimate cases are the first group—those who presented with Covid symptoms. As Dr. Tom Jefferson, the FDA and others have warned, PCR tests were not designed to be used randomly across general populations.
And these tests are not always reliable even in diagnosing symptomatic people. Without knowing the cycle threshold values of tests conducted, we have no clear data to identify true cases.
Over nearly a year, only two dozen of our Covid “cases” have been hospitalized. And even the people in that category likely included false positives. If a person was admitted to the ER due to a heart attack or stroke but tested positive for Covid, they were added to the county “case” tally and put in the Covid ward.
What is the real picture of Covid in our community? Of the 330 “cases” who received only a yes/no result from a PCR test that ran up to 45 cycles, how many test results were false positives? If the majority of people tested here were asymptomatic, how many of those with positive results were actually contagious?
Based on testing data the New York Times obtained from three states, only a tenth of the people counted as cases were true Covid positives; 90% were unnecessarily forced to isolate and submit to contact tracing. Jefferson County’s percentage of false positives may not be quite as high as those in Massachusetts, New York and Nevada. But without reviewing the Ct values of our test results, we simply do not know.
Why accurate case counts matter
In practical terms, being erroneously identified as a Covid case can have serious consequences. A false positive could result in your healthy teenager being quarantined for no reason, leading to suicidal ideation. Suicide rates have risen dramatically, especially among youth, since lockdowns were imposed.
Your own false positive might mean lost wages or damage to your business. Perhaps most harmful, though, is being stigmatized as a threat to other people’s safety. I know of people who felt perfectly healthy, but tested positive—likely false positives—and even after two weeks of quarantine, were treated like lepers by friends and co-workers afraid to be around them.
In a Daily Mail article, Dr. Tom Jefferson of the internationally acclaimed Cochrane Collaboration gives many examples of how people’s lives are being ruined by a similar testing regime in the UK:
“Last week I received an email from someone whose results have flip-flopped from positive to negative four times over two months, and another from a man who has been unable to see his elderly mother, isolated in a care home, because she continues to test positive week after week.” People, he says, “are at their wits’ end because they are testing positive for Covid-19 despite having recovered from their symptoms. Some never had symptoms in the first place but are still being told they have the virus long after any possible infection. They are anxious and confused. Their lives are on hold.”
At the extreme, being wrongly labeled a Covid case can kill you.
Say you are the person described earlier with no Covid symptoms and you have broken a bone. You are rushed to the ER and required to have a PCR test. A false positive result at a 45 cycle threshold places you in the Covid ward next to a contagious true-Covid-positive patient. Whereas your only actual medical issue is from your broken bone, you are now at risk of contracting Covid. And of dying— like the 80-year-old woman being counted as a Jefferson County Covid death. She was put in a Seattle hospital for complications due to surgery and is reported to have died from catching the virus there.
What has all this cost?
How much time, energy and resources have been spent for this massive testing program and the relentless propaganda campaign of ever-rising case numbers used to keep the public in fear?
What has been the true cost in Jefferson County? Much more than the money expended on 18,000+ tests and all the personnel involved. The impact on our community’s mental health, economic stability and social fabric is incalculable.
Dr. Tom Jefferson calls this deeply flawed testing program a “hugely expensive blunder”:
“I’d have to conclude that the official coronavirus figures have been grossly overstated, with all the damage that entails. Where appropriate we should carry out tests, but only in the context of symptoms, the date they first emerged, a history of recent contacts and any pre-existing medical conditions. I believe that Britain’s new-found testing mania is a retreat from properly conducted clinical medicine as well as from common sense. And that we are witnessing a triumph of herd thinking – an expensive one at that.”
Citizens have been terrorized week after week with alarming headlines about new case numbers, urging them to get their tests. Officials who have promoted this fear are deeply invested in the false story they have spun and the resources that have been wasted. No one wants to hear that they are responsible for such a massive error.
So the response is to shoot the messenger. Voices revealing the truth are censored, insulted, and vilified. In Jefferson County that is a coordinated effort between local media, the board of health, and our public health director.
We are now being told that censorship—the prohibition of free and open dialog—is justified. It’s for the greater good. These people are dangerous. And the more indefensible the narrative becomes, the more the censorship and attacks intensify.
PCR tests are being misused “to justify excessive measures such as the violation of a large number of constitutional rights,” writes Belgian physician, author and public health analyst Dr. Pascal Sacré. The assumption that a “positive RT-PCR test means being sick with Covid” is misleading, he says. Falsely equating positive tests with Covid cases is “the starting postulate, the premise of all official propaganda, which justifies all restrictive government measures: isolation, confinement, quarantine, mandatory masks, color codes by country and travel bans, tracking, social distances in companies, stores and even more importantly, in schools.” [source]
Are our leaders going to permit this misguided testing program to continue to fuel fear and inflict untold harm in our county? It is long past due for our local officials to put an end to this costly mistake.
by Dr. Rob Rennebohm | Feb 7, 2021 | General
As a pediatrician and pediatric rheumatologist who has published peer-reviewed articles on COVID-19, I would like to comment on the importance of knowing the Ct value at which a SARS-CoV-2 PCR test becomes positive. [The Jefferson County Health Department is not releasing this information. See our earlier article at this link. The Editor]
The PCR test for the SARS-CoV-2 virus is a good test when it is properly manufactured, properly conducted, used in an appropriate setting (e.g., in the evaluation of inpatients with COVID-like clinical features), and properly interpreted by carefully and fully taking Ct values into account.
It is not a reliable test when used in the screening of asymptomatic (or only mildly and non-specifically symptomatic) individuals, if the test is positive only after 33 or more cycles of amplification and this full information is not reported to patients and their physicians.
Ct = Cycle threshold; Ct = the number of amplification cycles needed before the test detects presence of viral material in a specimen. The higher the number of amplification cycles needed before detection of viral material occurs (i.e., the higher the Ct number), the lower the viral load and the less sick and contagious the person is likely to be.
If a test becomes positive after only 12 amplification cycles (i.e., positive at a Ct of 12), the viral load is very high—approximately 100,000,000 copies per microliter. [1-3] If the test becomes positive after 22 cycles (at a Ct of 22), the viral load is approximately 2,500,000 copies/mL. [4-5] If the test becomes positive only after 37, 40, or 45 amplification cycles, the result most likely represents either a false positive, or a true positive due to only a trace amount (less than 100 copies, even just 1-3 copies) of inert, non-contagious, “dead” SARS-CoV-2 viral debris (assuming the test is truly capable of always accurately identifying such a tiny amount of viral debris). [2, 6, 7]. Rarely, a positive test at a high Ct is identifying an asymptomatic person who has very recently become infected and might soon have a high viral load (low Ct), but this possibility can be evaluated by carefully following the person and repeating the test within 3-4 days, to see if symptoms develop and/or the Ct drops.
Unfortunately, it is very difficult to know with certainty whether a positive result at a Ct of 33 or higher represents a false positive or an accurately identified trace amount of SARS-CoV-2 viral material. The test was not designed to be reliably accurate after so many amplification cycles. When the test is used in an appropriate setting and the test is positive at a Ct of 30 or less, the false positivity rate is probably less than 4% (perhaps only 1-2%, as the test manufacturers claim). However, when the test is used in a surveillance setting and is “positive” at a Ct of 33 or higher (particularly at 37 or higher) the exact false positivity rate is currently unknown and likely to be quite high—probably as high as 70%. [6, 7]
Based on what is currently scientifically known, it is best (most accurate) to label any test result that is “positive” at a Ct higher than 32 as an “inadequately interpretable” result. It is not scientifically sound and, in fact, is misleading and harmful, to label people with a positive test at a Ct of 33 or higher as a “new COVID-19 case.” More accurately, they are people with an “inadequately interpretable” result who, furthermore, are unlikely to be infectious [2, 8]. Regarding this latter point, please see Graph 1 (after the References section), which points out that it is extremely unlikely that a person with a positive test at a Ct >35 is infectious.
For the above reasons, experienced PCR scientists recommend stopping the PCR test after 30 (or 32 at the most) amplification cycles, because positive results obtained after 32 or more cycles are unreliable (inadequately interpretable) [2] and are not associated with contagiousness [2, 8].
Unfortunately, to date, SARS-CoV-2 PCR tests have been reported only as being positive or negative, with no indication of how strongly or weakly positive. Although Ct results have always been available for each individual test (since the beginning of the pandemic), Ct results have not been routinely reported or used for clinical or epidemiological purposes. This has been the case throughout the USA and most of the world.
It has also been unfortunate that most SARS-CoV-2 PCR tests are set to perform 40, 45, even 50 amplification cycles in their effort to detect viral material. (This varies from one test kit to another—see Table 1 after References.) That is, if a person’s specimen is negative after 30 amplification cycles, further cycles are, nevertheless, performed (up to 50 cycles with some tests), looking for evidence of tiny amounts of viral material. Only if no viral material is detected after 40, 45, or 50 cycles (whichever number the test system sets as the stop point) is the test declared negative. Even if a test becomes positive only after 45 or 50 amplification cycles, it is declared a positive test (without any mention of the Ct value) and the person tested is declared a “new COVID case.”
The Jefferson Healthcare Lab uses the XpertXpress SARS-CoV-2 PCR test, which is set to perform 45 amplification cycles before stopping its effort to detect SARS-CoV-2 viral material.
When a person is told they have a positive SARS-CoV-2 PCR test, they deserve to know how strongly positive their test is and what their result means. Does their result mean they are carrying a huge viral load, are very contagious, and should be very worried about themselves and those with whom they have been in contact? Or are they carrying only a tiny amount of dead, non-contagious viral debris that represents no threat to them or others? Or are they in a pre-symptomatic phase, with a low viral load that could soon accelerate? Or does their result represent a false positive?
The Ct value at which a person’s test is positive can shed considerable light on the above critically important questions. But, again, to date, Ct values of positive tests have not been made available to patients, physicians, public servants, or the public.
Having emphasized the importance of knowing the Ct value at which a test is positive, it is important to also emphasize that there are limitations to the information provided by the Ct value. The Ct value is not a true quantitative test of viral load; it just provides a rough and indirect (but, nevertheless, very helpful) estimate (a good, educated guess) of what the viral load might be. It is true, too, that if the same specimen is tested with 3 different COVID PCR tests each might be positive at a different Ct value (e.g., at a Ct of 16 in one test, 20 in another test, and 22 in the third—but not at 37 or 45 in one of the three). For these reasons Ct values need to be interpreted with caution and in clinical context, particularly until more data on Ct values of positive tests have been collected and fully analyzed.
In the meantime, it is far better to have a COVID PCR test report that includes the Ct value at which the test was positive, than to have a report that only says positive (or negative) without any Ct information provided. Though imperfect, the estimate of viral load offered by the Ct value is far more valuable than no estimate at all, especially if the Ct value is carefully interpreted and placed into clinical context.
When in early November the CDC reported that 100,000 “new COVID cases” (meaning new instances of a person having a “positive” SARS-CoV-2 PCR result) were occurring per day in the USA, neither the individuals with the positive tests, their physicians, their public health departments, the CDC, the NIH, WHO, Johns Hopkins University, or the public knew what percentage of those 100,000 tests were positive at a Ct >32 and what percentage were positive at a Ct of 30 or lower—because, to date, the Ct values at which tests have been positive have not been reported or taken into consideration.
It would be enormously beneficial if we, as a nation, were to report, study, clinically use, learn from, and base public dialogue and public policy (at least in part) on the Ct values of positive tests. This would include retrospective and prospective reporting of the Ct values of all positive tests. We could at least start doing this in Jefferson and Clallam counties and, thereby, lead the nation in doing so. We would be doing the nation a great service.
Medically, morally, and ethically— individuals with positive PCR tests, as well as physicians, epidemiologists, public policy makers, and the public— deserve to know, and need to know, the Ct value at which a SARS-CoV-2 PCR test is positive. Without Ct information, interpretation of the number of “new COVID cases,” “new COVID hospitalizations” and “new COVID deaths” is severely compromised, as is public policy and the care of individual patients.
From now on, when a person is told that their SARS-CoV-2 PCR test is positive, they and their physicians would be wise to ask, “At what Ct value was the test positive?” And when the public is told that 100,000 new COVID cases have been occurring per day, the public and their public servants would be wise to ask, “What percentage of those 100,000 were positive at a Ct of 33 or higher (particularly a Ct of 37 or higher)?”
Such questions and their honest answers would facilitate healthy public dialogue and stimulate much-needed critical thinking—both of which are essential for successful resolution of the COVID-19 pandemic. True science and true democracy depend on such critical thinking and healthy, informed, public dialogue.
For further, more detailed discussion of Ct values, including caveats about Ct information, please see my original article, “The Importance of Knowing the Ct Value at which COVID PCR Tests are Positive,” which may be found on the “Notes from the Social Clinic” website: https://notesfromthesocialclinic.org/the-importance-of-knowing-the-ct-value-at-which-covid-pcr-tests-are-positive/
REFERENCES:
- Tom MR, Mina MJ. To Interpret the SARS-CoV-2 Test, Consider the Cycle Threshold Value. Clin Infect Dis. 2020 May 21: ciaa619. Published online 2020 May 21. doi: 10.1093/cid/ciaa619
- TWiV 640: Test often, fast turnaround, with Michael Mina. https://youtu.be/kDj4Zyq3yOA
- Your Coronavirus Test is Positive. Maybe it shouldn’t be. Interview with Michael Mina, MD. Published August 29, 2020; Updated September 17, 2020. https://www.nytimes.com/2020/08/29/health/coronavirus-testing.html
- Bryan A, Fink SL, Gattuso MA, et al., SARS-CoV-2 viral load on admission is associated with 30-day mortality. Open Forum Infect Dis. 2020 Dec; 7(12): ofaa535. Published online 2020 Nov 3. doi: 10.1093/ofid/ofaa535
- Perchetti GA, Nalla AK, Huang ML, et al. Validation of SARS-CoV-2 detection across multiple specimen types. J Clin Virol. 2020; 128:104438. doi: 10.1016/j.jcv.2020.104438
- Francesca F, et al. Detection of SARS-COV N2 Gene: Very low amounts of viral RNA or false positive? J Clin Virol. 2020 Dec; 133: 104660. Published online 2020 Oct 14. doi: 10.1016/j.jcv.2020.104660.
- Katz AP, et al. False positive reverse transcriptase polymerase chain reaction screening for SARS-CoV-2 in the setting of urgent head and neck surgery and otolaryngologic emergencies during the pandemic: Clinical implications, Head Neck 42 (7) (2020) 1621–1628, https://doi.org/10.1002/hed.26317
- Jaafar R, Aherfi S, Wurtz N, et al. Correlation Between 3790 Quantitative Polymerase Chain Reaction–Positives Samples and Positive Cell Cultures, Including 1941 Severe Acute Respiratory
Syndrome Coronavirus 2 Isolates, Clinical Infectious Diseases, ciaa1491, https://doi.org/10.1093/cid/ciaa1491
GRAPH 1: Percentage of positive viral culture of SARS-CoV-2 PCR positive naso-pharyngeal samples from COVID-19 patients. No sample that was positive at a Ct >35 had a positive culture. (Reference 18: Jaafar R, Aherfi S, Wurtz N, et al. Correlation Between 3790 Quantitative Polymerase Chain Reaction–Positives Samples and Positive Cell Cultures, Including 1941 Severe Acute Respiratory).
TABLE 1:
The number of amplification cycles that various commercial SARS-CoV-2 PCR Tests are set to perform in their effort to detect viral material:
- Gnomegen: 39 cycles
- GK: 40 cycles
- In Bios-Aires: 45 cycles
- Xpert Xpress: 45 cycles
- Luminex: 45 cycles
- Quest: 50 cycles
by Jim Scarantino | Feb 6, 2021 | General
The public has a right to know whether they can trust the COVID test results being used to destroy businesses and jobs, to curtail educational, community and religious activities and to exacerbate many of our already serious social ills, including substance abuse, domestic abuse, crime and suicides. An arrogant, “Because I say so,” is no longer acceptable. We are seeing public health officials and county commissioners finally speak against Governor Inslee’s arbitrary and unscientific dictates.
Citizens have the right to know how solid or flimsy is the testing data being used to extend lockdown orders now recognized as unfair and not based on sound science.
As explained in an article here by Annette Huenke, Jefferson Healthcare is using testing protocols that can return, in lay terms, practically meaningless positive COVID test results. We are not being told how many cycles were run on each reported positive “case.” Anything above 32-33 cycles or so is recognized as producing meaningless results (again, in lay terminology). Jefferson Healthcare employs a protocol that can run as many as 45 cycles on a sample until it gets a result or the cycles are completely run through, raising unanswered questions about how many of our “cases” were little more than meaningless test results.
It matters because people with only trace (again in lay terms–read the article for more precision) evidence of COVID, and with no symptoms or risk of transmission are being added to our numbers, Each additional “case” is used as justification to continue to inflict injury on our community and individuals with a senseless extension of the Governor’s ever-changing-but-never-expiring lock down order.
Private citizens have the right to ask these question. Disclosure of this information is routine in some states. It is mandatory in Florida. Stephen Schumacher is well qualified as an investigator of what should be a matter of public record. He understands data and knows the questions to ask. He graduated with honors in Mathematics from Harvard College and programmed funds transfer systems between Wall Street banks and the Federal Reserve before moving to Port Townsend in 1983. He has served as an officer for various community organizations such as the Food Co-op, Jefferson Land Trust, and the Northwest Nutritional Foods Association. He co-created The Port Townsend and Jefferson County Leader’s original online newspaper and programs shipboard stability software used by naval architects. He is a careful, rigorous researcher.
He has been asking important questions of Dr. Thomas Locke, Jefferson County Health Officer, for months, with no response at all. Recently, after publication of several articles here, Dr. Locke communicated with Mr. Schumacher, but still is not answering these questions. For that matter, neither is the Washington Department of Health. What we are getting is deflection and, at times, ad hominem jabs. This happened last year when Gov. Inslee was confronted with evidence that COVID death statistics included instances where people clearly died from other causes, such as being murdered. He deflected questions about these facts and insulted the research foundation that had uncovered this information in the DOH’s own records.
We are publishing the full exchange thus far of correspondence between Dr. Locke and Mr. Schumacher. The Board of County Commissioners has sometimes been in the middle of this exchange. The Clallam County Health Department has also been receiving the correspondence.
To fully grasp the importance of the details being discussed, we suggest reading Ms. Huenke’s article and Mr. Schumacher’s article published by Port Townsend Free Press, and the sources linked in each of those articles.
Mr. Schumacher to the Board of County Commissioners, a response and critique of Dr. Locke, 2/6/2021
Dear Jefferson County Commissioners,
I received the following emails from Dr. Locke responding to my
questions to you about PCR tests with high Cycle Thresholds.
Dr. Locke says the county doesn’t set “standards for what is
considered a positive PCR test” so “if you have an issue with Ct
values you should take it up with Washington DoH or the FDA.”
This passes the buck while ignoring things the county CAN do, such as
(1) direct Jefferson Healthcare to look for a PCR test with Ct cutoff
below 35 cycles instead of 45; (2) obtain the Ct value for each
positive test through PCR labs’ customer support when Ct is not
routinely reported as Florida DoH requires; (3) include Ct values
with case statistic reports, so our county can know how many cases
occurred at each Ct level.
Dr. Locke says Cts “add little of value to … the diagnosis of
active SARS-CoV-2 infection [since] they are more reflective of
specimen quality, viral load, and variations of lab technology.”
But “viral load” is directly relevant to infection diagnosis! The
hundred million virus copies per microliter at low Ct are far more
indicative of a true positive diagnosis than the trace viral debris
identified at Ct of 45. Even if the negligible quantity was due to
“specimen quality”, high Ct indicates a re-test is needed before
counting a positive test result as a COVID case.
Dr. Locke says “false positive tests … appear to be quite
infrequent with PCR testing, especially when a person has a
COVID-like illness”.
This may be true when Ct is low, but consider that “in three sets of
testing data that include cycle thresholds, compiled by officials in
Massachusetts, New York and Nevada, up to 90% of people testing
positive carried barely any virus… from 85 to 90% of people who
tested positive in July with a cycle threshold of 40 would have been
deemed negative if the threshold were 30 cycles”.
https://www.nytimes.com/2020/08/29/health/coronavirus-testing.html
Dr. Locke says false positives are infrequent because “we focus PCR
testing on people who are symptomatic”. But where is the data
showing most of our nearly 18,000 tests to date were on people having
relevant symptoms? Many asymptomatic county residents have sought
tests out of fear, and every hospital patient is required to be
tested even if their issues are not COVID-related.
It may also be that our county case count is as high as it is because
routine testing of many asymptomatic people has led to many high Ct
positive tests. The only way to know for sure is by reporting the
percentage of cases exhibiting symptoms and the Ct associated with
positive tests.
Though the estimate of viral load provided by Ct may be imperfect, it
is far more helpful than a bare positive or negative test
result! How could getting no information about viral load (or a wild
guess) be better than the rough estimate (or educated guess) provided
by a Ct value interpreted cautiously in a clinical context? People
have a right to know and should be trusted to know.
Yours truly,
Stephen Schumacher
Dr. Locke’s immediately preceding correspondence to Mr. Schumacher, copied to BOCC and others, 2/2/2021
Mr. Schumacher,
Hopefully, the bulk of your concerns were addressed in my response to
your long list of questions yesterday. Your notion that Jefferson
County case rates might somehow be reduced by applying a new
definition to PCR positivity is fanciful, at best, and delusional, at
worst. CT values are only one of many factors used to interpret PCR
test results. CT is merely a measure of the degree of amplification
of the viral genetic material present in the clinical specimen. As
previously mentioned, many factors can affect the amount of virus on a
swab. Additionally, labs vary in terms of protocols and testing
equipment and CT values can vary from lab to lab, even on identical
specimens. Far more important, from a standpoint of separating “true
positives” from “false positives” is the pretest probability of
infection. Most diagnostic tests will yield false positive if done on
people with very low risk of having the condition being tested for
(low pretest probability). The converse is true as well, if performed
on people with high pretest probability of infection, the positive
predictive value of a positive test result is much higher. This is
why we focus PCR testing on people who are symptomatic with COVID-like
illness and/or have close contact exposure to known cases of
infection. These are the Jefferson County cases you are speculating
might be erased by redefining CT thresholds — people who are acutally
symptomatic for COVID-19 or are household/workplace contacts of active cases.
The group that is more likely to have false positive results are those
who are being screened prior to surgical procedures or travel. This
is especially true if the person is asymptomatic and has no exposure
risk factors. Since 20-40% of COVID infection can be asymptomatic and
infection can be spread in the presymptomatic phase of illness,
preprocedure testing has its values but it does run the risk of
generating false positive results. This is completely independent of
the CT value you seem very interested in. When we suspect a false
positive result, we generally need to do two additional negative tests
to establish that diagnosis.
Your apparent belief that there is an epidemic of false positive COVID
tests is not supported by the facts. If anything, confirmed tests
dramatically underestimate the true COVID disease burden in a
community (by a factor of 5 to 10X in most studies). The reason that
CT values are not routinely reported by labs is that they add little
of value to the purpose of the test — the diagnosis of active
SARS-CoV-2 infection. They are more reflective of specimen quality,
viral load, and variations in lab technology. If you would like the
Washington State Department of Health or the FDA to revise their PCR
testing protocols you should take that up with them. Jefferson
County Public Health cannot serve as your intermediary in this
process. We have far more urgent duties to perform.
Sincerely,
Thomas Locke, MD, MPH
Jefferson County Health Officer
Dr. Locke’s Correspondence to Mr. Schumacher, copied to BOCC and others, 2/1/2021
Mr. Schumacher,
Cycle threshold values on PCR tests performed to detect SARS-CoV-2 are
not routinely reported by laboratories to health departments or the
person ordering the test. The Washington State Department of Health
establishes standards for what is considered a positive PCR test and
is reportable as a notifiable condition. The local health officer has
nothing to do with establishing CT parameters or any other diagnostic
lab parameter. If you have an issue with CT values you should take it
up with Washington DOH or the FDA. Jefferson County Public Health
does case investigations and contact tracing of all positive tests
reported to Washington State and available to us through a
confidential on-line registry known as WEDSS.
The fact that a thermal cycler can perform up to 45 amplification
cycles does not mean that ALL tests are amplified to that degree.
Samples are cycled until a signal is detected or they have undergone
the maximum amplification of the testing protocol. Samples can have
high CT values for many reasons — poor sample quality, degradation of
the sample during transport, low viral levels in the person being
tested, and testing late in illness when fragments of non-replicating
virus can be detected. And it is certainly true that high CT values
correlate with lower transmission risk (assuming adequate sample
collection and specimen transport). Setting standards for FDA
approved diagnostic tests is a federal regulatory function. States
set standards for notifiable conditions such as SARS-CoV-2 infection.
County health officers, local boards of health, county boards of
commissioners, and public hospital district commissioners have nothing
to do with these decisions.
Again, if you have grave concerns that the Washington State Department
of Health is using scientifically indefensible criteria for
determining which COVID-19 PCR tests are positive, please share your
expertise and concerns with them. These criteria are not set by
county health officers or local hospital districts. Nor do we
manufacture or license the PCR machines that are used to test
diagnostic specimens for SARS-CoV-2. We rely on these tools along
with our case investigations (looking at exposure risk, symptom onset,
and other risk factors) in assessing cases. False positive tests can
occur with any diagnostic technology. They appear to be quite
infrequent with PCR testing, especially when a person has a COVID-like
illness or a recent exposure to a confirmed case. If your goal is to
support the pandemic denialism that Ms. Huenke promotes in the “Port
Townsend Free Press” article you reference, I could not disagree more.
With the spread of more transmissible variants of SARS-CoV-2, the
social cost of pandemic denialism is increasing. If sizeable numbers
of people indulge in the wishful thinking that attempts to control
COVID-19 transmission are unnecessary, it is only a matter of time
before variant strains become predominant. We still have time to
avert this future or at least slow it enough to allow widespread
vaccine deployment. I urge you to join the community fight against
COVID-19 and stop attacking those who are working long hours trying to
protect their community from the worst public health emergency in the
last 100 years.
Sincerely,
Thomas Locke, MD, MPH
Jefferson County Health Officer
Stephen Schumacher to BOCC, 2/1/2021
Cc: Board of Health; Tom Locke; Allison Berry, Clallam County Health Officer
Subject: New hope for “negative cases” before Feb. 14
Dear Jefferson County Commissioners,
Watching the Zoom of this morning’s BoCC meeting, I noted that Dr.
Locke did not answer or even address any of my questions at bottom,
so they are all still on the table. I’m mystified by his
mischaracterization of well-documented concerns over 90% false
positive rates at high cycle counts as “nitpicky” and his
easily-refuted opinion that PCR tests are “highly accurate”.
Philip Morley observed that Jefferson Healthcare handles only a small
percentage of our county’s PCR testing, with most conducted by UW and
others. If so, that raises the additional question:
7) What Cycle Threshold is used by each organization performing PCR
testing in our county, and approximately what percentage of testing
is done by each organization?
Because of the critical importance of the cycle count in evaluating
the significance of a positive PCR test result, both pieces of
information need to be reported to individuals as well as in overall
county statistics.
Dr. Locke’s report began by warning about a tripling of cases with 26
new ones last week if I heard correctly. But what are the cycle
counts of these new cases? It makes a huge difference whether they
were found positive after 20 amplification cycles or after 45 cycles.
My interest is getting at the truth, not politics. But today’s
meeting seemed concerned about county cases showing percentage
improvements before a Feb. 14 deadline One way to achieve that in a
hurry might be to re-examine recent cases and reclassify any that
were incorrectly counted due to amplification cycles higher than 33,
then continue using that rule for new cases. Not only would that be
the right thing to do, it might achieve the “negative cases”
[Commissioner] Greg [Brotherton] ruefully joked are needed!
Yours truly,
Stephen Schumacher
Stephen Schumacher to BOCC, 1/31/2021
Cc: Board of Health; Tom Locke; Allison Berry, Clallam County Health
Officer; news@ptleader.com; PT Free Press
Subject: Accountability for Jeffco’s 45-Cycle Threshold PCR Test
Dear Jefferson County Commissioners,
On September 2, 2020, I sent the following Public Comment to the
Jefferson County Board of Health and Health Officer Dr. Tom Locke:
“Per the August 29 New York Times report [of 90% false positives at
40-cycle threshold], I’m concerned about the criteria used to
determine confirmed cases of COVID-19 in Jefferson County. Do all
these cases exhibit symptoms, or are “cases” being equated to
positive test results? If the latter, what percentage of cases
exhibit symptoms? Are positive test results being recorded using PCR
tests, and if so, what is the Cycle Threshold value used for these tests?”
I never received any answers to these questions nor have seen them
addressed by Dr. Locke in the press.
Last week the Port Townsend Free Press reported that Jefferson
Healthcare is “using a PCR assay with a 45-cycle threshold, well
beyond the outer limits of reliability.”
https://www.porttownsendfreepress.com/2021/01/25/is-jefferson-county-h
ealth-department-overstating-covid-case-numbers/
This revelation raises various accountability issues, including:
1) Why did our county have to wait nearly 4 months to learn about its
45-cycle threshold from a fortuitous Public Records Request?
2) Since Dr. Locke was also Clallam Health Officer until recently, is
this same unreliable 45 Ct test also in use throughout Clallam County?
3) Was the choice to use this 45 Ct test ever discussed and approved
by the Jefferson County Board of Health or County Commissioners? If
not, was it ever even reported and its significance explained to them?
4) Does Dr. Locke or anybody else keep statistical track of
cumulative cycle counts for positive tests and resulting cases in our
county, or is this info unavailable or being ignored? Could this
information be regularly published in the media, or at least be made
available upon request?
5) Does our county always order a second test following a positive
PCR result, and if not, how often and on what basis? Are all
positive tests treated as COVID-19 cases regardless of symptoms, and
if not, how often has high cycle count been used to discard extremely
weak positive test results?
6) How many county residents have been reported as cases,
quarantined, and contact-traced based on cycle counts above 33, when
the CDC shows “it is extremely difficult to detect any live virus in
a sample above a threshold of 33 cycles”?
Yours truly,
Stephen Schumacher