by Annette Huenke | Oct 31, 2022 | General
BERRY: nothing but hope for vaccine efficacy
“The biggest thing that we can do to protect ourselves
and our community as we move into the fall is to get vaccinated,
both with our Covid boosters and get our flu shot.
That’s how we protect ourselves, our neighbors
and our health care system as we move into the fall.”
(9-26-22 BOCC meeting)
FACT CHECK:
By now, it is an indisputable fact that the Covid jabs don’t prevent infection or transmission. Admit it — just about every jabbed person you know has had Covid, at least once. The “vaccines” don’t protect granny or the grandkids. On the contrary, latest research shows that they degrade the human immune system and lead to negative efficacy (more on that later). One can only wonder if our public health officer has caught whatever it is that President Biden has.
Delusion and speculation have been the bedrock of nearly all Allison Berry’s pronouncements, like this one from the June 7th, 2021 BOCC meeting wherein she performs the art of magical thinking on the survival of two patients who’d just been in ICU with severe cases of COVID-19:
“In both of those cases, we think the primary thing that has kept them alive was they were vaccinated. They were both incredibly ill prior to contracting COVID-19 and very likely would not have survived if they were not vaccinated.”
Two people with life-threatening comorbidities nearly died, officially from the virus, after their jabs. But they were saved by the jabs. Uh huh.
When the spectacular failure of the new mRNA therapies could no longer be bluffed, senior players got busy reworking the script. Had it not been so tragic, it would have been comical to witness pharma apologists’ gyrations to concoct a new narrative, eventually landing on the wobbly claim that the toxic brews lessened symptom severity and the chance of hospitalization and death. None of those outcomes were part of the trial endpoints, but never mind. The controllers turned up the spin machine to convince the public that the data supported those claims.
Associate Editor at the British Medical Journal (BMJ), Dr. Peter Doshi had already revealed in an October 21, 2020 editorial that this was nonsense:
Peter Hotez, dean of the National School of Tropical Medicine at Baylor College of Medicine in Houston, said, “Ideally, you want an antiviral vaccine to do two things . . . first, reduce the likelihood you will get severely ill and go to the hospital, and two, prevent infection and therefore interrupt disease transmission.”7
Yet the current phase III trials are not actually set up to prove either (table 1). None of the trials currently under way are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus.
Five months later, US Congressman Thomas Massie publicly took the CDC to task for lying about the efficacy of the jabs, in order “to strengthen vaccine confidence.” Our public health officer spent years at university learning this stock in trade, and she does not divaricate.
The Medical School Incubation Process
Allison Berry Unthank graduated from Johns Hopkins University in 2013. According to her LinkedIn account, Allison Berry is a Medical Doctor who also earned a Masters in Public Health with an epidemiology and biostatistics focus (2010-2011). Her bachelors degree was in biochemistry and music.
In 2018, while she was working for the Jamestown S’Klallam Tribe in the addiction medicine department, she was appointed county health officer by the Clallam County Board of Health. In July of 2021, authority over Jefferson County citizens was added to her plate by our BOH.
Just eight years out of university, she assumed outsized medical authority over 109,000 residents of the north Olympic Peninsula.
Healthcare provider statistics aggregator Vitals.Com (where she gets very mixed reviews) cites Allison Berry’s specialty as family medicine. They then list as proficiencies, one would imagine — weight loss, contraception, family planning, checkups, influenza and — immunization. Family medicine began revolving around “immunization” after the vaccine makers were absolved of liability for harm from their products in 1986 — just one year after our young medical marvel was born.
Note the color alert in the background: Be Afraid, Be Berry Afraid!
Dr. Berry was anointed as our new public health officer by the BOH at the July 15, 2021 meeting. Oddly, she strove to convince that nest of pharma conformists that she would somehow deliver an element of neutrality to her new position:
“I take public service incredibly seriously and I take the role as an independent scientific advisor for this region very seriously.”
“I’m hopeful that I can bring a lot of strength to the position and that commitment to scientific independence.”
Berry does not have a degree in epidemiology, thus is not an epidemiologist, as some of our commissioners have claimed. She is not a scientist, as she herself intimated in the comments above. Above all, she is not independent. Education at the Johns Hopkins University system is akin to being cultured in a petri dish. Step outside the medium and you shall perish. Berry has brought years of medical-industrial complex indoctrination to her position, not strength.
Medical universities are largely funded by research grants from pharma and pharma-captured government agencies. Medical doctors are not educated about vaccines, nutrition or natural cures. They are taught that vaccines are safe and effective, and that deviating from the CDC schedule is verboten. They are taught to “persuade, not inform” to address vaccine hesitancy. PTFP editor Ana Wolpin provided an incisive overview of the pharmaceutical industry’s grip on medical schools in the local Vaccine Study Group’s 2017 publication, Vacci•nation, for which she was graphic designer and primary author.
Johns Hopkins is only one of those bought medical schools, but it may be the apex in terms of worldwide influence, as they have teamed up with globalist vaccine pushers like the Gates Foundation and the World Economic Forum to “war-game” pandemic readiness tabletop exercises since 2001, including Event 201.
Say it, say what you said, say it again
Many will recognize that maxim as a time-honored public speaking device used to hammer home a message. It’s effective. More than the mRNA jabs, by a long shot. (Sorry, that was irresistible.) Pharma mavens, including our own, have been deploying that tactic, shamelessly, throughout this charade and it’s been memorialized in various walk-it-back videos people like Fauci and Birx would prefer to forget.
Two years later, confessions reveal: “I knew these vaccines were not going to protect against infection.” – Dr. Deborah Birx, July 2022.
White House Covid response coordinator Dr. Deborah Birx testified in a June 23, 2022 US Congressional hearing that she knew of Covid re-infections as early as December 2020.
Asked “When the government told us that the vaccine couldn’t transmit it, was that a lie or was that a guess?” Birx replied, “I think it was HOPE that the vaccine would work in that way.”
Now that the big foot has come off the “pandemic” accelerator, and federal and state funds are drying up, the county budget demands that Dr. Berry’s oversight of JeffCo be reduced to 12 hours a week. The Monday morning perpetual fear campaign euphemistically known as “updates” delivered at the weekly BOCC meetings for the last 2-1/2 years, broadcast to the most receptive audience one could hope for on local radio station KPTZ (it was their most popular “program”), will now happen monthly.
Seeing the Overton window closing, Berry laid it on thick at the October 17th BOCC meeting, pitching the ever more urgent need to be up to date on your boosters because another two elderly, chronically ill jabbed souls needlessly passed away because they weren’t jabbed enough. Loath to miss an opportunity to condemn the unjabbed, she tossed out one of her baseless warnings that we’re only seeing severe disease in the “unvaccinated,” then went on to un-say that and press on with her Birxian fantasy that the heralded new jabs (same contents as the old jabs plus a big puff of hot air from an 8-mice “study”) might prevent transmission. If enough people take it.
“We are not seeing a rise in severe disease at this point. It is still too early to tell what the effect will be of the bivalent vaccine on transmission, but we are hopeful it will reduce transmission, but we haven’t seen enough uptake yet. We definitely encourage more folks to go out and get vaccinated. It is really important to reduce transmission as we move into the fall.”
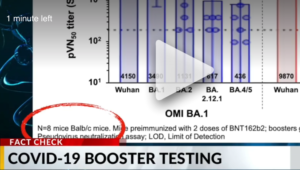
The 8-mouse study, on which pharma pinned its argument for approval of the new bivalent booster, was a complete failure in stopping transmission. When the mice in the Moderna trial were challenged with the Ba.5 variant which the Ba.5 booster is supposed to protect against, all eight of them became infected with Covid. Every last mouse.
The first five jabs that we pinned our hopes on may have let us down, but this next one, jab number SIX — same technology, for which once again there is zero evidence of ability to reduce transmission, only a study that says it does not — this one really really really just might work if we only can get enough uptake… if we repeat our mantra to “encourage more folks to go out and get vaccinated” enough times. So says our hopeful spin doctor.
Negative ‘Vaccine’ Efficacy
Dr. Berry and her ilk continue to attribute to Covid — with singular diagnostic proof coming from the dubious PCR test — deaths which were imminent in the chronically ill, elderly and immunocompromised people (and were most likely hastened by the jabs). Since this population-wide phase III clinical trial began in December of 2020, evidence has mounted that the gene therapies are actually weakening immune systems, exacerbating and reactivating existing or latent conditions like herpes and cancer, and causing new disease. Vaccine spike proteins have been found in shingles blisters!
The more jabs you take, the more likely you are to get Covid. The jury has returned the verdict on negative efficacy. You would think that having their “expert” noses regularly rubbed in the colossal failure of these clot shots to prevent “break-through infections” in just about everyone who has taken them would give one pause to fall back and regroup.
Nope. That would be unwise. Even the New York Times counseled against that crazy critical thinking business. Instead, dig the heels in deeper to hedge your bets on keeping the scared silly scared silly. There’s great benefit to that tactic, as that team will bat for you till the end. It’s certainly working in much of Jefferson County.
Enough of Allison Berry’s evidence-free pronouncements. Show us the Science!
Our young, unseasoned public health officer instituted the first dine-in vaccine mandate in the country in September 2021. Her power was given lift by her predecessor Tom Locke, license by our county commissioners, and full support from the communities’ population they’d already managed to frighten out of their wits.
That science-free, oppressive and likely illegal diktat descended with tremendous cost. Clallam and Jefferson County restaurateurs lost tens to hundreds of thousands in unrecoverable income, their employees lost wages and endured unrelenting stress, and the unjabbed — whose first amendment rights were fully crushed — lost trust and good will that may never be regained.
As the walls come tumbling down, we can only expect a mad scramble to retain the authority they’ve wielded over the last nearly three years. We have been warned.
————————————
by Kincaid Gould | Oct 30, 2022 | General
BERRY on pharma fraud during vaccine trials:
“[I have been] asked if there have been any valid
concerns raised about Pfizer clinical trials,
about poor design or data falsification…
And the answer is no, actually.”
(2-14-22 BOCC meeting)
FACT CHECK:
Last February, Dr. Berry answered a question about whether or not there was the possibility of fraud in Pfizer’s (still ongoing) clinical trials. “[T]he answer is no, actually,” she said.
According to Dr. Berry, these “were very high quality trials,” and they have been “very heavily scrutinized.” She also pooh-poohed the suggestion that any degree of fraud could have occurred, proclaiming that no “valid concerns… about poor design or data falsification” had been documented.
Enter Brook Jackson
A Certified Clinical Research Professional with almost two decades of experience in a clinical trial setting, Brook Jackson joined Ventavia Research Group in 2020 as a Regional Director. Ventavia had been contracted to carry out clinical research on Pfizer’s vaccine before Jackson signed on, and she began noticing issues as soon as she started work there.
When she brought concerns such as “failure to preserve blinding,” “vaccine dilution errors,” “patient safety issues,” “enrollment and injection of ineligible trial participants,” and “falsification of data” to her supervisors, no actions were taken to remedy the situation. Jackson ultimately related the issues to the FDA, but not without repercussions: just hours after talking with the FDA under supposed confidentiality as a whistleblower, Ventavia contacted Jackson to inform her that she was “not a good fit” for the company and that she was fired.
Brook Jackson was fired from Pfizer contractor Ventavia after bringing safety concerns to the attention of her superiors and the FDA. Watch the BMJ’s 6-minute video of her story.
Refusing to be silenced, Jackson proceeded to file a legal complaint against Ventavia and Pfizer under the False Claims Act (FCA), contending, among other wrongs, that “Pfizer… represented that the clinical trial would comply with all applicable laws and regulations [but that] Defendants violated… multiple FDA regulations when conducting the clinical trial, rendering this certification false.” The 81-page complaint is accompanied by 29 exhibits spanning an additional 551 pages, including emails and text messages, Pfizer source documents, photos of HIPAA and other violations during clinical trials, blood draw data, and lists of errors and deficiencies.
The FCA allows whistleblowers to sue the defendants on behalf and/or with the intervention of the federal government. Suits brought under the FCA are sealed so that the government can investigate the allegations without the defendant’s knowledge. After a period of several months had elapsed with little communication from the government (more on this in a moment), Jackson decided to share her information with the British Medical Journal (BMJ), one of the world’s preeminent and most highly regarded medical publications, despite her case being under seal.
On November 2, 2021, the BMJ published an investigative piece focused on the incident at Ventavia, noting that “Revelations of poor practices at [Ventavia] raise questions about data integrity and regulatory oversight.” The BMJ’s publication enumerates half a dozen specific concerns identified by Jackson:
- Participants placed in a hallway after injection and not being monitored by clinical staff
- Lack of timely follow-up of patients who experienced adverse events
- Protocol deviations not being reported
- Vaccines not being stored at proper temperatures
- Mislabelled laboratory specimens
- Targeting of Ventavia staff for reporting these types of problems.
In its interview with Jackson, the BMJ included a photo Jackson took of a “plastic biohazard bag [that] contained used needles” which should have been disposed of in a sharps box.
(Meta’s fact checker Lead Stories quickly responded by decrying the coverage done by the “British Medical Association’s news blog.” Citing as evidence to rebut the claims of fraud were spokespeople from both Ventavia and Pfizer, the former alleging that “no part of [Jackson’s] responsibilities concerned the clinical trials at issue.”)
Jackson’s case was sealed for more than a year, until early 2022 when the government elected not to intervene in the case. Pfizer filed a motion to dismiss the case in part on the grounds that “the complaint alleges FDA was the victim of ‘fraud’ even though the agency has known about [Jackson’s] allegations for years, has not withdrawn the [vaccine] approvals in question, and continues to express confidence in the data underlying those approvals.” Therefore, even if the court were to find that Pfizer had committed fraud, it wouldn’t matter because the government would have bought their product anyway.
On October 4, the federal government then made a curious move when it submitted a statement of interest supporting Pfizer’s motion to dismiss the case: “[Jackson]’s complaint lacks factual allegations that would support a plausible claim that Ventavia’s clinical trial violations masked problems with the vaccine that were so serious that FDA would have withheld or withdrawn its authorization of the vaccine had it known the truth, such that Pfizer’s subsequent claims for Government payment for the vaccine could be rendered ‘false or fraudulent’ under the FCA.”
Jackson’s attorneys responded on October 27, characterizing the government’s response as an “unusual pleading.” “[T]he government sought this court’s extraordinary seal powers over this case for a substantial time period because of how seriously they took the pleadings as fully legally sufficient as plead…. Had the government truly believed… that [Jackson]’s complaint was devoid of evidence, they would never have required such ample time to investigate.”
Jackson’s attorneys insinuate that if the government was aware of fraud by Pfizer, it could potentially abuse its power to seal the case in order to keep the case out of the public eye — something it succeeded in doing for almost a year before Jackson took her evidence to the BMJ. One can only wonder how many people would have chosen not to take the vaccine if they had known what Jackson knew when she knew it.
As of the publication of this Free Press article, the court has still not ruled on the motion to dismiss.
Jackson’s claims of wrongdoing have received a lot of press, but they aren’t the only reason to suspect fraudulent activity in Pfizer’s clinical trials.
Who is Maddie de Garay?
Earlier this month, Dr. Berry received a simple question: “Who is Maddie de Garay?” In a long-winded response where she not only failed to identify the young teenager by name, but also avoided describing any of the many problems de Garay suffered (and continues to suffer from) immediately after receiving her second Covid-19 shot as part of Pfizer’s clinical trials, Berry also managed to digress from the topic and harp on such things as “right wing talk radio.”
Maddie’s mother, Stephanie de Garay, says that “[i]n less than 24 hours of her second dose, [her previously] healthy and vibrant 12-year-old had a severe systemic adverse reaction.” In her mother’s words, Maddie is now “in a wheelchair, receives all her nutrition and medicine through a feeding tube, cannot control her neck, has constant stomach, back, neck and body pain, vision problems, tinnitus, can’t feel from the waist down, allergic reactions, dysautonomia and… her condition is declining.”
Maddie’s parents have given numerous interviews and even testified on what happened to their daughter (see videos here and here).
Stephanie de Garay testifies on her daughter’s behalf in Washington: “She had severe chest pain. The way she described it, it felt like her ‘heart was being pulled out of her neck.’”
In Pfizer’s report on its trial, there was one participant listed with an ongoing adverse event at the trial cutoff date. Maddie’s adverse events were ongoing when the trial ended, meaning that either the description of that participant, who was “eventually diagnosed with functional abdominal pain,” referred to Maddie, or that Pfizer omitted Maddie from its report to the FDA altogether. Pfizer deemed the adverse event unrelated to the individual’s injections.
Berry sent warm thoughts Maddie’s way over the airwaves noting that she “hope[s] she gets well,” but only after hammering down that “[i]t’s very difficult to say whether or not this girl was even in the trial.” This is an easily contestable claim. Perhaps one of the most convincing pieces of supporting evidence is a recorded phone call between Maddie de Garay’s parents and Dr. Robert Frenck, lead author of the study on the safety of Pfizer’s vaccine in adolescents.
When Dr. Berry then attempted to quash Maddie’s story by suggesting that “it’s just really unclear that those concerns are related to the vaccine,” it became obvious why she had opted not to describe Maddie’s condition in any detail — her paltry ‘lack of causality’ argument is utterly unconvincing and talking about Maddie’s reactions could have potentially fueled local ‘vaccine hesitancy.’
Even if Maddie’s declining physical condition was not a result of vaccination, the situation still merits investigation. To date, this has not occurred, and the de Garay family has been left to pay hundreds of thousands of dollars in medical bills out of pocket. Maddie was one of 1,131 participants in her trial who received the shot, meaning that her extremely severe adverse reaction occurred at a rate of around 884 per million.
Pfizer is accused of fraud not only in the US, but the EU, too.
These are two of the most notable instances of fraud allegations in the context of Pfizer’s Covid-19 shots, but not the only ones.
Concerns have surfaced following the court-ordered release of Pfizer’s clinical trial documents requested under FOIA by Public Health and Medical Professionals for Transparency (PHMPT). A non-profit organization comprised of international scientists and medical experts, PHMPT advocates for data relied upon by the FDA to license Covid-19 vaccines to be publicly available for independent review and analysis. After the FDA attempted to keep the data sealed for 75 years, and Pfizer intervened to also delay its exposure, the court ordered release at a rate of 55,000 pages per month starting on March 1, 2022.
With so much data being released, many eyes have been necessary to pore over the many documents. The FDA has still not yet finished producing all of Pfizer’s data, so it can be difficult to draw certain conclusions until it has released all of its publications.
Just recently, the European Public Prosecutor’s Office announced an investigation into vaccine contracts signed by the EU and Pfizer, opening up the possibility of fraudulent financial activity.
And let’s not forget Pfizer’s track record of paying out multi-million dollar settlements for fraudulent practices (see here, there and everywhere), including what was the largest health care fraud settlement in the history of the US DOJ.
Silencing the alarm and refusing to acknowledge that there even might be fraud going on in Pfizer’s clinical trials as Berry has attempted to do is disingenuous, although perhaps unsurprising given that her incessant exaltation of the vaccines over the past two years has married their two fates together.
———————————-
by Ana Wolpin | Oct 29, 2022 | General
“Jefferson doesn’t have the level of population
immunity that others do, because it did such a good job
controlling the virus before.”
— Dr. Allison Berry
_______________________________
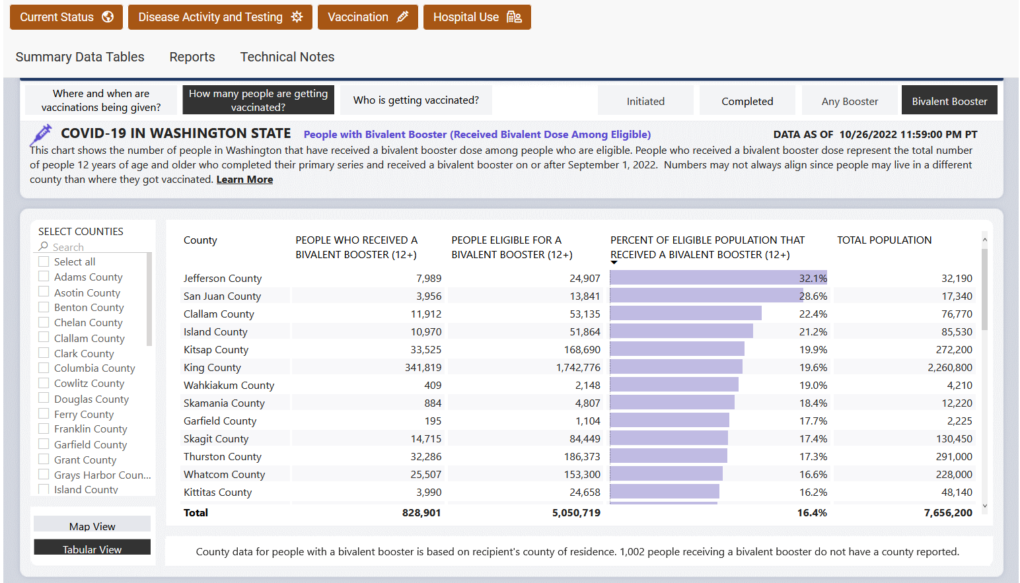
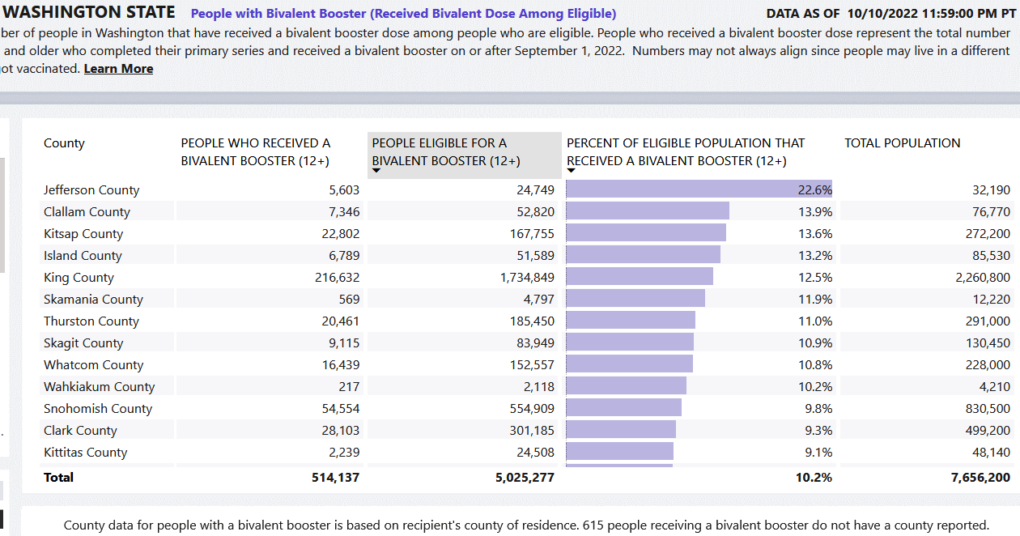
Public Health Officer Dr. Allison Berry has presided over a pandemic response that boasts the most draconian mandates in the state. Primary series vaccination uptake is reported to be 80% in Jefferson County, the third highest statewide. And at 32.1%, uptake of the bivalent booster is double the state average.
The result is that JeffCo is currently identified as one of the highest-risk counties in Washington, often with some of the worst case numbers and surely the greatest ongoing fear quotient.
Wrap your head around the bizarre non-sequitur (above) of why we have the worst level of immunity statewide. It is precisely because her destructive mandates and high vax uptake were so successful, she explains, that we are now the most vulnerable.
It is absurd pronouncements like this, delivered with impunity, that make it so difficult to narrow down Berry’s disinformation statements to a short list.
Despite her mantra that the shot will protect you, we need only look at all the double-vaxxed and boosted public figures championing these leaky injections who have succumbed to the virus. Often more than once. Dr. Anthony Fauci and President Biden top that list nationally, and locally are County Commissioners, Port Townsend’s City Manager, most of the City Council, and members of the Board of Health.
Nonetheless, embracing Einstein’s definition of insanity, Berry’s response is that more of the toxic mRNA spike protein brew will fix that. Even as the two-year fear narrative dissolves in admission after admission after admission of false information perpetrated on a traumatized public, Berry still continues to push for more dangerous shots in arms and for useless masking that destroys our human connections.
As with our year-end TOP TEN 2021 Spin Doctor Disinformation Statements, four of us have contributed to this series — the editorial team (Annette Huenke, Stephen Schumacher and Ana Wolpin), plus Free Press contributor Kincaid Gould.
Part One begins with a fact-check of Berry’s inconsistent claims about v-safe.
_______________________________
BERRY on the CDC’s cover-up of v-safe data:
“V-safe [is] actually publicly available datasets.
Nobody had to be sued to release them because
they’re already publicly available.”
(10-20-22 BOH meeting)
FACT CHECK:
The above two assertions about v-safe are outright lies. Curiously, on October 10 Berry told the county commissioners a different story: “There is an anti-vaccine group that has been suing the CDC to get access to this raw data.”
Spinning the story one way for the commissioners, then doing a complete about-face for the Board of Health (BOH) ten days later, she lied that “nobody had to be sued.”
“I think it’s important to kind of review that for folks,” Berry riffed. At that Oct. 20 meeting she insisted that v-safe data had always been publicly available. “They are public access datasets,” she assured the BOH. “You can go in right now and track your side effects related to getting vaccines.”
What is v-safe and why has the CDC avoided transparency?
V-safe is a phone app developed to “tell CDC about any side effects after getting the COVID-19 vaccine.” It was designed to monitor adverse reactions, to capture problems following the experimental shots initially identified in pharma’s trials. The American public was told that v-safe would detect safety signals more rapidly and reliably than VAERS and that all v-safe data collected would be transparent.
Contrary to Berry’s assertion to the Board of Health that these are “are public access datasets,” the opposite has been true. Not only has the CDC hidden v-safe data for most of the past two years, the agency spent a year playing legal games — dodging FOIA requests and multiple lawsuits — to keep the data under wraps.
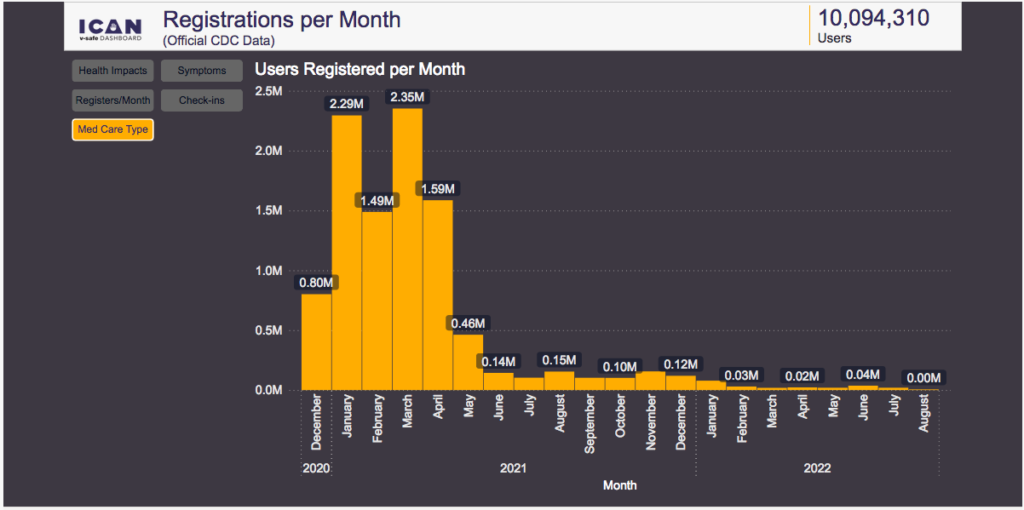
As reported in my March 2021 Free Press article, information from the v-safe Active Surveillance system was publicly disclosed for only the first five days of America’s Covid vaccine rollout, December 14-18, 2020:
“Over those five days, more than 5,000 “Health Impact Events” immediately following injections were identified. On December 18 alone, 2.79% of people who received first dose shots—3,150 out of 112,807—used this smartphone app to report reactions so severe that they were ‘unable to perform normal daily activities, unable to work, [and/or] required care from a doctor or other health professional.’”
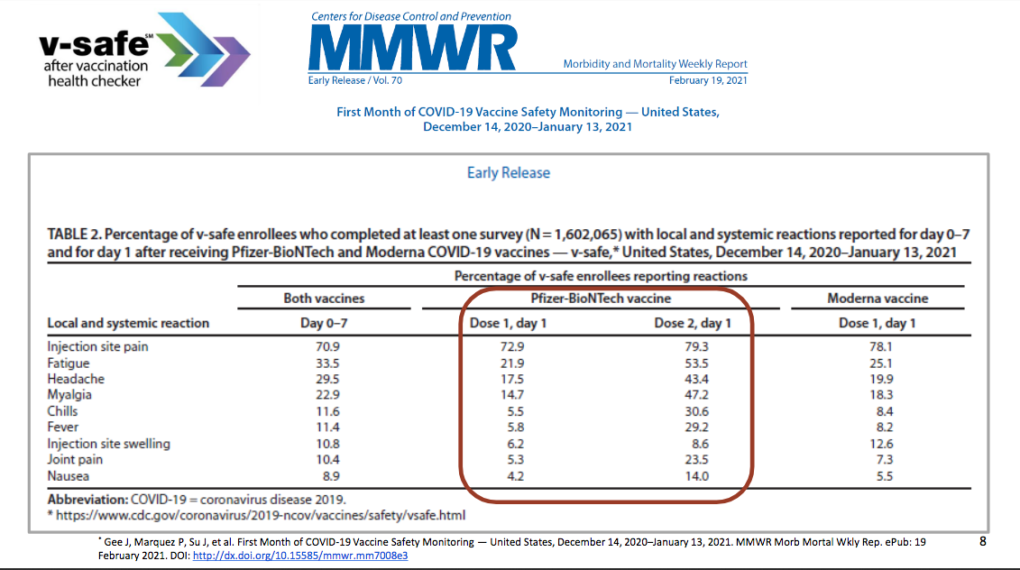
When initial v-safe reporting undermined pharma’s Safe and Effective narrative that the federal government had committed over a billion dollars to promote, the data went dark. Only one other snapshot from v-safe — titled “First Month of Covid-19 Vaccine Safety Monitoring” — can be found in CDC materials. In a 2021 “Safety Update” justifying the shots, the CDC included this table below. It showed high percentages of “local and systemic reactions” like headaches, fatigue, fever, myalgia and joint pain, the reactions health officials spin as “proof the vaccines are working.”
Those signals alone were significant enough to raise red flags. More important is what the CDC avoided disclosing. What this first-month report didn’t show were severe adverse events, emergency room visits, hospitalizations, and other serious outcomes which, as revealed below, were formidable. Following that incomplete cherry-picked snapshot, for nearly two years all v-safe information was then covered up.
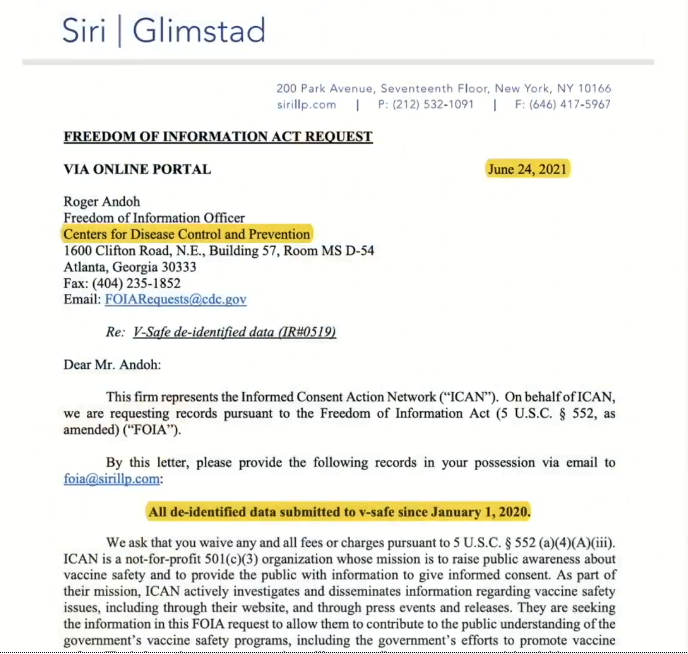
In June 2021 Aaron Siri, lead counsel for the nonprofit Informed Consent Action Network (ICAN), filed a Freedom of Information Act (FOIA) request for release of the CDC’s V-safe data.
6/24/21 FOIA request for “All de-identified data submitted to v-safe since January 1, 2020.”
“Mandating that millions of Americans inject a product for which they cannot hold the manufacturer liable if the product injures them demands complete transparency, especially when it comes to releasing the data underlying the product’s safety. FOIA exists precisely so that Americans can obtain transparency, and, in this case, obtain the data which supports the CDC’s claims to intensive safety monitoring.”
After a response from the CDC that the data requested “could not be located,” an appeal was filed in August 2021. A second, reworded FOIA request was submitted on behalf of ICAN in September.
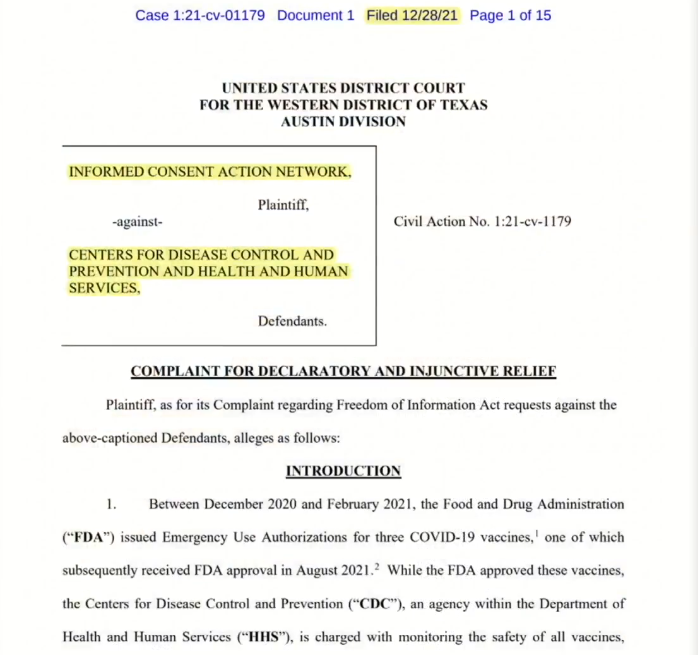
When that request was also sidestepped, a lawsuit was filed in December.
Page 1 of first lawsuit from ICAN petitioning for release of the CDC’s v-safe data.
The CDC continued their attempts to hide the data. A third FOIA request was submitted in April 2022, and in May another lawsuit was filed. It had been almost one year since the first FOIA request was submitted.
The second lawsuit declared that ICAN “intends to make all v-safe data immediately available to the public so that independent scientists can immediately analyze that data.” It referenced the need “to address serious and ongoing issues with the vaccine program, including waning immunity [and] adverse reactions.” Preventing independent scientists from reviewing this data, the suit argued, was “at best, irresponsible and unethical.”
CDC Ordered to Release Data
While Berry lied to county commissioners that “nobody had to be sued” for v-safe data to be made public, the record shows that it took multiple FOIA requests and two lawsuits to force the CDC’s hand. Fifteen months from the initial FOIA request and twenty-one months after the vaccine rollout, a court order required the CDC to provide the v-safe data on or before September 30, 2022.
When forced to comply with the court order, the CDC said the v-safe files would be released to ICAN, but claimed they lacked the ability to post the information on their own website. After a year of maneuvering to hide this data, the agency disingenuously wrote that they had planned to post the data on their website, but had “not yet completed the technical and administrative processes required to post data.”
V-safe files were sent to ICAN just one month ago, at 6 pm on September 30. What the CDC claimed they lacked in “technical and administrative” proficiency to do for 21 months, ICAN’s modest staff accomplished over a weekend. On October 3, three days after the grassroots nonprofit obtained five digital files comprised of initial data from more than ten million users, ICAN launched a user-friendly web dashboard allowing the international science community and other members of the public to view the data themselves and perform interactive searches on that data.
ICAN, not the CDC, is responsible for making this information accessible, nearly all of it (86% as shown above) reported to v-safe in the first six months of the rollout. The multi-billion dollar public agency charged with safeguarding our health instead used its formidable resources to block release of v-safe reports.
What did the CDC not want us to see?
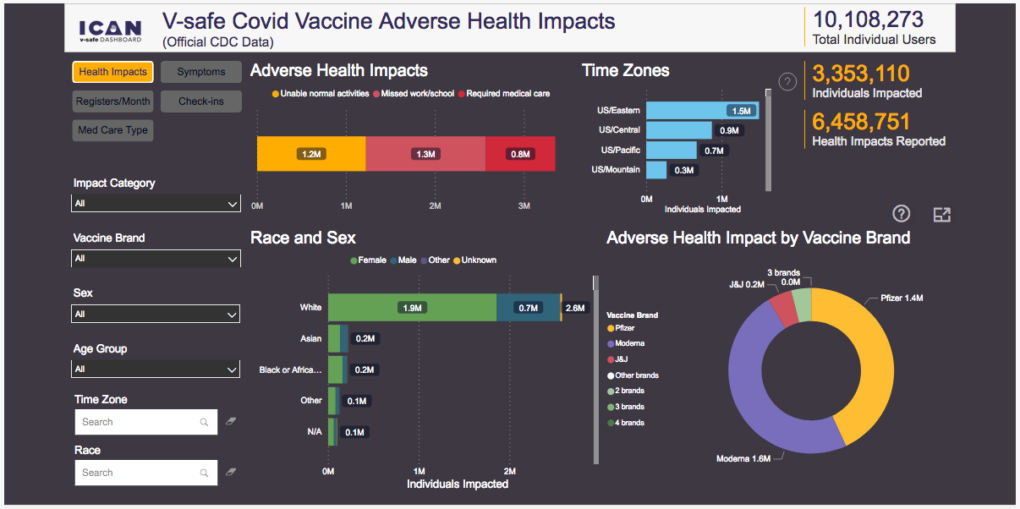
Unsurprisingly, signals of damage from these shots — which public health officials like local mouthpiece Dr. Allison Berry continue to deny — are alarming. The percentage of adverse health impacts following Covid vaccination reported to v-safe over 21 months is more than ten times the 2.79% seen in the December 18, 2020 snapshot, on day five of the rollout.
Of the 10 million+ individual users who participated in v-safe after their shots:
- 71.3 million symptoms were entered, an average of 7 symptoms per user
- 6.4 million adverse health impacts were reported
- 33% (3.35 million) were unable to perform normal daily activities, unable to work, and/or required care from a doctor or other health professional
- 7.7% (782,913) had a health event so severe it required medical attention, emergency room intervention, and/or hospitalization, most of those events requiring multiple visits
Contrary to Berry’s lies, the CDC not only had to be sued for access to this critical data, they spent more than a year fighting to prevent its release. Had this data seen daylight, as fanfare leading up to the rollout had promised (“this information helps CDC monitor the safety of Covid-19 vaccines in near real time“), Emergency Use Authorization of the shots could never have remained justified.
The entire story can be seen, with all supporting documents, at Aaron Siri Breaks Down CDC’s V-safe Data.
V-safe data is still not available on the CDC’s website. It can only be accessed through ICAN’s interactive dashboard.
This is not the end of the story.
While incriminating enough on their own, the five files a court order forced the CDC to release one month ago were incomplete. ICAN discovered through further litigation that an important category of the reports was not included in the files they received. The agency continues to stonewall on disclosing all v-safe records. More lawsuits are pending.
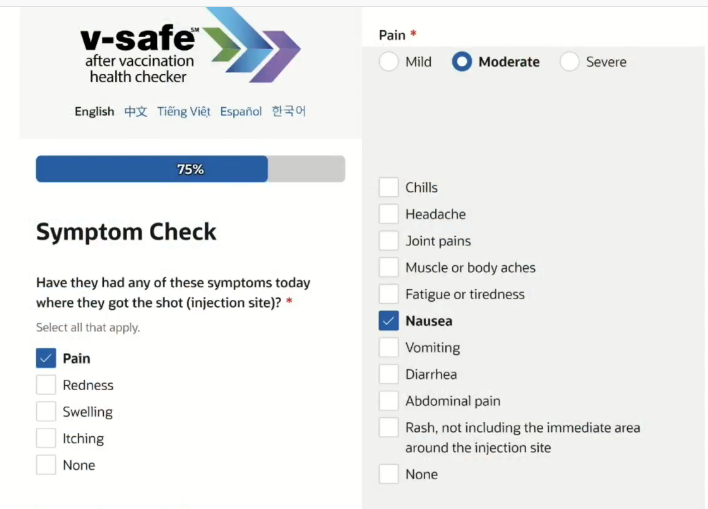
The v-safe app provides simple checkboxes for symptoms experienced following vaccination, like the local and systemic reactions shown in the CDC’s first month Safety Update (12/14/20 – 1/13/21) — headaches, chills, joint pains and other symptoms that are said to be proof the shot is “working”.
The app also includes check-the-box fields for users to report if they required medical attention, emergency room intervention, and/or hospitalizations following the shots, as revealed on ICAN’s dashboard.
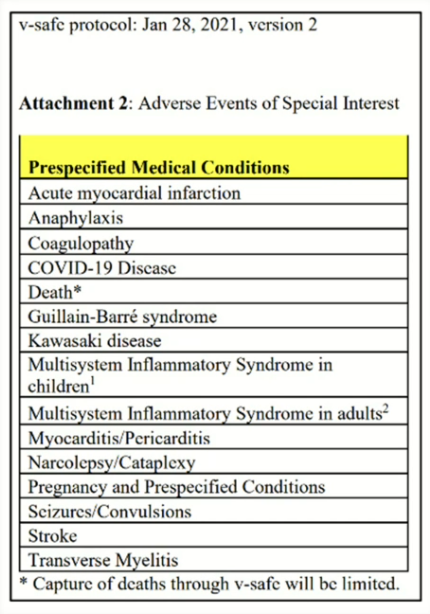
V-safe does not provide checkboxes for “Adverse Events of Special Interest,” issues the CDC knew from early trials were much more serious concerns. These “Prespecified Medical Conditions” are shown in the v-safe protocol attachment below, but omitted from the app.
The sometimes deadly medical issues we have been seeing in unprecedented numbers — like acute myocardial infarctions (heart attacks), anaphylaxis, seizures, Guillain-Barre syndrome (paralysis), strokes, pregnancy problems and myocarditis/pericarditis — were known to be caused by the mRNA injections when v-safe was developed. But the CDC avoided delineating them on the app.
Instead, the only way to capture reports of those issues was in “open fields” — empty boxes where users could type in additional details. Anything other than check-the-box local and systemic reactions which generally did not result in medical intervention had to be reported by the user as supplementary information.
Despite the extra effort it took, of the ten million registered users in the v-safe database, over six million open field entries were submitted. These open field reports were not included in the data the CDC turned over to ICAN and are yet to be revealed. The further lawsuits in progress expect to obtain that information.
Berry’s tangled web of disinformation
The CDC designed the v-safe app to make it easy to report symptoms people were told to expect from the shots, but obscure the devastating outcomes that would undermine the public’s confidence in their Safe and Effective narrative. This obfuscation has supported their lie about the incidence of severe adverse events, and provided cover for health officers like Berry to parrot that disinformation:
“Severe side effects from these vaccines are incredibly incredibly rare,” she told the Board of Health during her v-safe review, “on the order of less than 10 per million doses delivered.”
After falsely assuring the BOH that v-safe data has always been publicly available, and lying that no one had to sue to get it, Berry lamented that “unfortunately, anti-vaccine groups have now gotten access to those datasets and are now using them and twisting the numbers in them to spread misinformation about the vaccines to suggest or argue that they are less safe than they actually are.”
In her erratic, loquacious web of disinformation — yes, there was a lawsuit / no, no one had to sue — she insists that there wasn’t a lack of transparency, just that the data had fallen into the wrong hands. She provides no proof that numbers were “twisted”, just blithely makes unsubstantiated pronouncements that anti-vaxxers are spreading misinformation.
Anyone can now review and analyze the CDC data for themselves through ICAN’s online portal.
And Berry’s claim that severe side effects are less than ten per million — incredibly incredibly rare — is belied by 7.7% of v-safe users reporting they required medical attention, emergency room intervention, and/or hospitalization after their shots. That translates to 77,000 — not 10 — per million serious adverse reactions following the experimental injections.
It is the CDC and spin doctor Berry doing the number twisting. And with six million open field v-safe data entries still to come — information that shot recipients had to be motivated to report in their own words — our glib, dismissive health officer has a whole lotta twisting ahead to maintain her crumbling disinformation narrative.
_______________________________
by Brett Nunn | Oct 27, 2022 | General
Summer is over. The rains have begun. I am back at my desk.
While we were enjoying the fine weather, our federal and state governments have continued with their plans to protect us from Covid. Let’s play a little good news/bad news and find out what they have been up to.
Good News! On August 31st the FDA authorized the new, fast-tracked, Covid boosters by Pfizer, Moderna and BioNTech for adults and children. The fast tracking was determined to be necessary to get ahead of the constantly mutating virus because past efforts took too long to produce effective substances.
Bad News! It was only tested on mice. Eight mice.
Good News/Bad News? They only needed to test it on mice because much of the data used to develop these fast-tracked shots came from the previous mRNA vaccines that the pharmaceutical companies, and our government, have told us — come on everybody, let’s say it together and make Allison Berry happy — are “safe and effective”.
Spoiler alert: this is sarcasm, but it is factual. I have paraphrased this information in effort to speak the truth plainly. If you think I am making this up, feel free to fact check by reading through the FDA document yourself.
We continue.
Good News for Pharma/Bad News for Parents
In what looks a lot like an end run around the many massive state-level protests against adding the Covid shot to the vaccines required for children to attend school, parents found the following in their news feeds on Thursday, October 20th.
Today, CDC’s Advisory Committee on Immunization Practices (ACIP) recommended updates to the 2023 childhood and adult immunization schedules, which includes incorporating additional information for approved or authorized COVID-19 vaccines. CDC only makes recommendations for use of vaccines, while school-entry vaccination requirements are determined by state or local jurisdictions.
How long before Washington State’s Board of Health reverses their decision from April 13th of this year, and makes the Covid shot mandatory to attend public school, stating that they “are just following CDC recommendations”?
If you don’t think this could happen, I point you to the continued medical tyranny of Jay Inslee as demonstrated in Directive of Governor 22-13.1 dated August 5, 2022. The Governor’s emergency powers were supposed to end on October 31; not true if you are a current or future state employee.
Here is the heart of the directive (bold emphasis mine):
To address this continuing threat and ensure the health of our workforce, I am directing a permanent COVID-19 vaccination condition of employment requirement for state executive and small cabinet agencies as follows:
- New Employees. As a condition of employment, all new employees of state agencies must be fully vaccinated against COVID-19, as recommended by the U.S. Centers for Disease Control and Prevention (CDC).
- Current Exempt Employees. All current exempt employees must be fully vaccinated.
As defined by Directive 22-13.1, an employee is “up to date” with their COVID-19 vaccination when they have received all doses in the primary series and all boosters recommended for them by the CDC Advisory Committee on Immunization Practices.
Just in case loyalty to Jay Inslee isn’t enough to assure compliance, the directive also authorizes the state Office of Financial Management to incentivize state employees to remain fully vaccinated.
On September 21 the Seattle Times revealed that a tentative deal between the governor and the Washington Federation of State Employees Union includes a $1000 bonus for each state employee receiving a Covid-19 booster shot. The cost of this bonus to state taxpayers has been estimated at close to $41 million.
Back at the federal level, why was this CDC approval necessary?
Was it because the federal government was concerned for our children’s health?
Or could it be that once the Covid shots are recommended for the list of official childhood vaccines by the CDC, there is no longer any legal liability for these corporations?
Direct from the Health Resources and Services Administration’s covered vaccines webpage:
The National Vaccine Injury Compensation Program (VICP) covers most vaccines routinely given in the U.S.
For a vaccine to be covered, the Centers for Disease Control and Prevention (CDC) must recommend the category of vaccine for routine administration to children or pregnant women.
The National Childhood Vaccine Injury Act of 1986 created the National Vaccine Injury Compensation Program (VICP), a federal government managed, no-fault alternative to the traditional tort system providing compensation to people found to be injured by certain vaccines.
The funding for this program comes from an excise tax on all vaccines administered across the country.
The latest information I could find that attempted to evaluate the effectiveness of this program was from a 2014 General Accountability Office report that calculated an average time to adjudicate claims at 3.5 years. Imagine how well the program is working now with the VAERS report listing 1,442,261 adverse effects just for Covid shots?
Could there also be a profit motive involved in being approved to the childhood vaccine list, a guaranteed income stream created for these pharmaceutical companies from now until well into the future?
In what has to be pure coincidence, only hours after the CDC recommendation, Pfizer management, on a call with holders of Pfizer stock, announced a 400% increase in the price of their Covid booster. They had been charging our government $30 a dose. Now that private insurance will be paying, Pfizer will be requiring $110 to $130.
Let’s end with some good news.
On Friday, October 21, the day after the CDC recommendation, the Informed Consent Action Network, ICAN, announced they will fund a legal challenge to any state that mandates the Covid-19 vaccine to attend school. That same day the governors of several states — and just in case you are planning a move, let me list them here: Florida, Virginia, Wyoming, Utah, Oklahoma, Iowa, Alabama, Tennessee, Missouri, South Dakota, Montana, South Carolina, Ohio, Arkansas, Georgia, Idaho — announced that regardless of recent CDC recommendations, they will not be mandating Covid-19 vaccines for school attendance.
Now is not time to sit back. Chris Reykdal, Washington State’s Superintendent of Public Instruction has been clear in his statements that he wants to mandate the Covid-19 vaccine for school attendance. He has been clear that this will be a statewide decision and no district can opt out.
Keep talking to your political representatives, find them here. Keep making phone calls (360-236-4110) and sending emails to the State Board of Health. Make it clear that the October 20th CDC recommendation changes nothing. If there is even the slightest doubt in their mind that this shot might not be safe and effective for our kids, then they have a moral obligation to keep the Covid-19 vaccine off the list of Washington State’s requirements for attending school.
— UPDATE —
This promotion was sent to PTSD parents after 10pm on Thursday, Oct. 27th. This is how desperate they are. Back in the day, our parents taught us to never take candy from strangers…
by Stephen Schumacher | Oct 23, 2022 | General
Jefferson County will be alone in its own private State of Emergency if commissioners approve its 13th temporary Covid-19 response policy emergency declaration at their October 24 board meeting. Meanwhile, Washington State and all its other counties (including neighbor Clallam) will have discarded their emergency declarations as of October 31.
County residents have been under the grip of multiple overlapping federal, state, county, and city emergency rules since both Jeffco and Port Townsend declared a State of Emergency on March 16, 2020, joining the February 29 state and March 13 federal declarations.
These unprecedented emergency lockdowns were originally sold by former Jeffco Health Officer Tom Locke and others as short-term measures to “flatten the curve” so it “does not overwhelm medical services,” which White House Coronavirus Response Coordinator Deborah Birx recently admitted was an evidence-free deception to “make these palatable” while “I was trying to figure out how to extend it” since “I didn’t have the numbers in front of me yet to make the case for extending it longer, but I had two weeks to get them.”
In fact, there never appeared “any widespread over-utilization of hospitals, especially in locations with little or no lockdown” (except arguably in New York nursing homes when its governor drove up deaths by forcing them to admit covid patients for six weeks).
A careful peer-reviewed cost/benefit analysis found the emergency “lockdowns have had, at best, a marginal effect on the number of Covid-19 deaths. … The costs were at least thirty-five times higher than the benefits. The reasonable conservative case is that the cost/benefit ratio is around 141 … Lockdowns are not just an inefficient policy, they must rank as one of the greatest peacetime policy disasters of all time.”
So the goal posts for lockdowns and emergency declarations kept moving as each old justification became discredited, eventually landing on little more than public health case-detection funding imperatives, perpetuation of Emergency Use Authorizations for the mRNA spike protein injections, and convenient ramping up for any future actual emergencies.
Public Comment About Extending Jeffco’s Emergency
That brings us to the County Commissioners’ October 17 meeting, whose agenda centered on discussion and potential action “In the Matter of Adopting a 13th Temporary County Policy Based on Emergency Response to the Covid-19 Pandemic”, about which I expressed the following Public Comment:
| I saw that Jefferson County may be keeping its emergency orders even after the other counties and the state lifts them on October 31, and personally I would really urge you not to do that. For one thing, that would be putting you out there special doing this unlike the other diligence from the other counties.
I understand that according to our health officer, “Jefferson doesn’t have the level of population immunity that others do, because it did such a good job controlling the virus before.” And there may be cases now and there may be cases in the future, but I’m not quite sure that constitutes an emergency.
If things happen during the winter, then maybe at that point one could consider calling it an emergency. Part of it is, I really would like us to normalize.
Forgive me for putting it this way, but for your electoral prospects, a lot of information has been coming out that makes the wisdom of these lockdowns look suspicious. To the extent you’re standing out there as the only county doing this thing, that allows you to be saddled with this label of being the “Lockdown Commissioners” or having done it above and beyond what other counties have done. Whereas if you’re just following the same actions as everybody else, at least you’re acting in a more safe way about all of this.
Another thing… a lot of stuff has been coming out in the news, like the European Parliament hearing Pfizer say they hadn’t done any testing on transmission for their vaccine, which was obviously part of the original narrative about it.
You’ve got countries around the world — Denmark, Norway, Australia — abandoning a lot of these recommendations for kids to have this vaccine, so things are changing and the narrative is shifting insofar as what the appropriate guidance should be.
We just had this V-Safe data dump, which shows 33% of their 10 million injections having pretty bad effects from the vaccine. Florida just did an analysis showing 84% increase of cardiac deaths for men under 40 in the first 28 days, so basically advises men under 40 and kids not to take the vaccine and everyone to be informed of these risks.
So you could almost say that this is becoming the emerging guidance. |
Commissioner Responses to Emergency Comment
Commissioner Kate Dean responded:
| One of things I’m most pleased about as we move into this endemic phase, we can start to heal some of the things that have cursed our country and communities. I think we knew all along this was a grand experiment; none of us had ever been through anything like this, and we’re all doing our best. I think it will be years before we understand what was effective and what was the right choice.I feel some hope that the things which have divided us for the last few years, that we can at least all say: we tried, we’re doing our best, we did well in this community. I don’t have regrets, but I’ll say we learned every step of the way.
Our conversation last week will be continued this afternoon regarding the emergency order. I have some concern about continuing it, mostly because I feel there’s a bit of a “crying wolf” situation: If we continue it, we perpetuate the sense of emergency, and then, where there actually is an emergency, it’s harder to rally folks to respond as such.
But I trust very much that the staff who are dealing with the administrative end of this think there’s a lot of benefit in keeping it in place to revisit in a few more months, in part because it’s hard to get stuff going again, so if we were to rescind it, then getting it back in place if we have a surge just takes capacity, when Public Health and the Department of Emergency Management have less capacity.
So I’m going along with staff’s recommendation. We’ll have more discussion about it today, but I anticipate we’ll go ahead with keeping it in place.
But I share your concern; I worry it’s a little disingenuous myself. But it’s a tool for administrative purposes, and we’re not doing any sort of lockdown. Obviously we’re all here today, and we’re glad to have the public back! |
Commissioner Greg Brotherton responded:
| I’m on the screen here today because covid is still with us. I’m on day 6 of my second positive test. While it was a very mild case, we still as a county have to deal with the reality that there is a lot of transmission, I assume over 400 per 100,000 in our community.
And some of the levers that emergency order for us are really critical to come up with extra pay for staff so we can maintain services, and also take care of them so they can stay home when they’re sick.
I’m also feel like it it’s a little bit disingenuous, and we’ll have a robust conversation I’m sure at 1:30, but I’m also like Commissioner Dean inclined to take the staff recommendation and just keep it on a little while longer, not as a lockdown, but to make sure we still have those levers available as we continue to deal with it, as I can attest with firsthand experience. |
Commissioner Heidi Eisenhour responded:
| I’m still evading covid, full stop, thankfully! … I was saying last week, we put all this stuff in place, so what happens if we rip the Band-Aid off now, with the potential cases happening in Europe, that Dr. Berry has been talking about, and how we’ve tended to follow the trend with our cases going up after cases in Europe in the past.
Personally, I know more people with covid right now than I ever have. And so, I don’t feel it’s time to stop having the precautions in place that we do, especially how the things we put in place affect the team here in the county for human resources issues. So It’s something we are going to have more of a conversation about this afternoon. |
Health Officer on Emergency and Everyday Powers
Following Health Officer Allison Berry’s community update, Commissioner Brotherton asked her:
| Where does the requirement to wear masks in health situations come from, could you remind me? |
Berry answered:
| It’s currently a mandate from the state. So there is an order from the Secretary of Health, and the Secretary of Health’s orders extend past the declaration of emergency.
That’s probably worth digging into a little bit. So health officers and secretaries of health always have the ability and authority and obligation to control infectious diseases regardless of states of emergency. Governors only have that authority when a declaration of emergency is in place.
So after October 31, the Governor doesn’t have the ability to issue orders around the pandemic, but health officers still do. We always have had that authority, we will continue to do so. Secretaries of health do too.
Many folks didn’t know we existed before the pandemic, but we have always been here! So if there was, for instance, a measles outbreak, we would issue health orders around that.
And so, as long as we’re still seeing high rates of covid transmission, we’re likely to see health orders related to that, but they’re more targeted now than they used to be, because we’re in a different phase of the pandemic.
And that one most critical space is health care. We need people to be able to see their doctors, and not get covid from that interaction. And so that’s where we are still requiring masking. Longterm care facilities also fall under that space, because people can’t choose whether or not they need to live there. And it’s really important to protect them in that space. |
Brotherton followed up about the emergency resolution:
| We’re going to be considering our 13th emergency resolution about covid this afternoon, and I’m wondering if you had a chance to look at it, whether you weigh in favor of keeping our emergency resolution or adding a 13th?
We’ve talked a little and had public comment today about it being disingenuous to call it an emergency as we move into an endemic phase. And it does seem a little strange, at the same time, there’s still a lot of important levers that it opens up to us to use. As I can attest, covid is still very high in our community. |
Berry answered:
| Yeah, it’s certainly a challenge to figure out how to move in a seamless way into this endemic phase and not lose all the gains that we’ve made as a community. And I think that’s where these kinds of emergency declarations come in.
The biggest thing that the local emergency declaration makes available is the ability to rapidly fund certain situations or make certain control efforts available.
But again, the emergency declaration doesn’t actually have a lot of bearing over whether or not, for instance, I can issue a health order.
And I think that’s where sometimes people end up having strong feelings about the emergency declaration is that thought that we would no longer have public health authority. And it actually has no bearing on that.
What it does is allow us to fund covid test, or potentially move forward something like the Department of Emergency Management responding to a covid outbreak. So it allows us a little more flexibility in responding to things.
I think it was appropriate, for instance, the federal goverment did just announce that they extended their emergency declaration so that we can continue to use some of the tools we need to fight covid through the fall.
It’s a complex decision whether or not to maintain it. But I think it’s useful to have those tools available and only use them when we need them, but it’s good to have that option. |
Public Comment After Emergency Wordsmithing
Commissioners returned in the afternoon to wordsmith their potential 13th emergency declaration together with public health staff. That draft would then be taken to the closed County Covid Coordination meeting on October 21 for further work. Afterwards I gave another Public Comment:
| I really appreciate you all wanting to honor staff, and if you stop these orders now, you’d have to ramp up and all — I grok that.
But what are the pluses and minuses here? I heard from the health officer that the big advantage was that the emergency declaration would allow getting funds, for example, to pay for additional covid testing and management.
I feel like a lot of this is sort of redundant stuff that is already being covered elsewhere. So there’s funds for more testing?
Why exactly is Jefferson County in a special condition compared to other counties, if we’re the only county that’s going to be doing this? I also heard that it was because we have more cases.
We also had one death recently, which I think was somebody in her 80s with lots of comorbidities who had been vaccinated and boosted but not fully. That’s also a situation in which who’s to say she died from the covid or died from all these other conditions.
So the main thing is the cases. Is this really an emergency any more? I do feel we’re in the endemic stage and not the pandemic stage.
I do feel like it’s disingenuous, as I’ve heard from others to try to be applying emergency things for something that is really just a casedemic here.
It’s not lots of deaths. It’s not the hospitals being overburdened. It’s just lots of cases.
And part of the reasons for all these cases is all the testing. So in a sense, if you had more funds from having this emergency order, then you could have more testing which could possibly provide more cases and make things seem to be more like an emergency.
So I’m concerned that we’re in this walking-on-eggshells mode, where — oh my gosh! — we just had a case, now we’ve got to shut down the whole workplace or have everybody be masking, changing, doing things in different ways.
In a way, I personally feel like it would be better to step back, not have it so easy that we’re just continuing the state of emergency.
Why not just basically say, like every other county is doing, say: Okay, it’s really not an emergency any more.
It’s a matter of concern that we need to be watching; it’s not an emergency. If it is an emergency in the future, then we can at that point make a decision and ramp up.
And then that’d be due diligence rather than it being this eggshelly thing, where on the turn of a dime, we’ll be back in this mode and you’ll never be able to feel you can normalize.
One other thing I’ll toss out: Jefferson County is different in one other way: I saw that there’s 22.6% bivalent boostering, which is more than twice the 10.2% in all the other counties in this state.
Who’s to say, I mean we have a correlation here, not a causation necessarily, between the boostering and the additional cases in this town. We’ve also been told by our health officer we don’t have the same level of population immunity as everyone else. So who knows?
But let’s take a step back and wait and see. |
Commmissioner Dean responded:
| I also came at this from the pluses and minuses, and like you heard me say earlier, I was afraid of the “crying wolf” scenario.
But what I couldn’t get to are what the negatives were. There are some positives that are potential positives, like not having to go through this whole process again.
Should we decide that we are in a state of emergency in a couple of months as we see numbers rise potentially, or if there are funding opportunities that we want to be eligible for, or just need to be able to respond in a true emergency fashion — you see that it takes us a long time!
Our process is very deliberative and includes a lot of people. On Friday, our staff will be meeting again. And so that’s where I felt like the negatives just aren’t there.
I appreciate that we’ve softened the language and really tried to not overstate things in this version, so I’m still happy to move it ahead at staff’s recommendation. |
Commmissioner Brotherton responded:
| I think you may be getting hung up on the word “emergency” like I did as well. And I think this is really just about the preservation of the temporary standards that we have.
I’m supportive of taking this to staff and seeing if everyone agrees, if we can get a consensus from the county coordination meeting this Friday.
I don’t see (as Kate said) any negatives from this. It just allows us to keep paid covid leave, which is critical for some of our staff. I’m in favor of moving this forward to county coordination. |
Commmissioner Eisenhour responded:
| I know covid has hampered all the departments, and now we’re needing to reduce the hours that the transfer station’s open because of capacity issues. It’s not tied to this policy, but it’s tied to people being sick and our county family.
I think taking away tools for managers to provide our team with what they need when they need it – it doesn’t feel like the time for that right now.
But the line of questioning that I had at the beginning of this session, where I was trying to unpack whether there was another place where we could take care of these policy matters … what I heard was that there’s not. So that further shores up my support for us continuing this conversation. |
Commissioner Candidate Kelbon’s Emergency Response
On October 19, Ben Montalbano asked County Commisioner (District 3) candidate Marcia Kelbon this question:
| If you were the County Commissioner now would you vote to extend the Emergency Authorization Act, now before the board? Many of us voters are not sure about you stand on community imposed mandates. |
Candidate Kelbon’s response:
| I do not see a need or defensible justification for a continued state of emergency. There are continued county employee protections that best be addressed by permanent employee policies.
To elaborate, I am surprised that this is even being considered at this point and that the three commissioners have expressed support for an extension.
I highlight county employee protections such as extended sick leave because that is the reason they most discussed, but they acknowledge that this could be addressed through their employee manual.
The other reason stated often is that it is a lot of work to put an emergency measure back in place if there is a surge. Work avoidance is not a reason to limit liberties.
The deputy prosecuting attorney also noted that the current emergency ruling avoids the need for competitive bidding for OlyCap – indefensible.
If there is a surge, people can choose to mask and/or boost if they choose. We need to be out of a police state and get on with life, with individuals and businesses making their own health decisions. |
Government by Law or by Emergency
Pushing back against Health Officer Berry’s maximalist view of her own powers, her public health order on September 2, 2021 requiring indoor restaurant/bar patrons to produce vaccination papers was inapplicably based on WAC 246-100-040:
This quarantine law provides narrow emergency detention powers to health officers for up to 10 days over infected persons posing serious and imminent risk, but only after a long series of provisions and recourses have been exhausted — none of which in any way applied to or authorized Health Officer Berry’s open-ended discriminatory regulation over restaurant/bar business practices, requiring them to demand HIPAA-protected private health information from their patrons.
Our counties’ restaurant vaccine mandate was a pure example of illegal emergency power overreach and the dangers of governance not by laws but by lawless “emergency” orders. Anything goes in an emergency — which is not a good thing.
Emergency declarations risk replacing everything good about our government — laws, rights, and due process — with lawless orders by unaccountable executives and unelected health czars.
They are meant for genuine short-term physical emergencies like earthquakes, and if used to replace normal government indefinitely under the pretext of long-term conditions like flus and climate change, such perpetual emergency takeovers are indistinguishable from totalitarian coups.
———————————
“In the end it’s very simple:
Emergency powers are just another name for lawlessness.
You can be a nation of rights and laws, or a nation of emergency.
You cannot do both.”
– el gato malo