by Ana Wolpin | Oct 30, 2021 | General
Do you know of local people who have been injured by
(or died from) the Covid injections?
You’re surely not hearing about vaccine injuries or deaths from any other local media. Obituaries about previously healthy residents who died following their jabs never mention that significant detail. Their obits simply say “passed unexpectedly,” or their deaths are attributed to contracting the Covid virus after being fully vaccinated.
Take the 60-year-old woman who died in May, only a week after she got her second shot. Her passing was denied to be a vaccine death by our county health department and instead claimed as a Covid death from the virus (see “New Wrinkle in Jefferson County’s ‘Fourth’ COVID Death“).
In the winter of 2021 I wrote about the vaccine-induced death of a friend’s aunt (“Death by Injection?“). Previously in good physical health, from the day she was vaccinated with the Pfizer experimental mRNA shot she rapidly began to lose her ability to function. Within a few days she was “having trouble sitting up straight,” and by day seven “she no longer could feed herself.” Day eight, “she was unable to get up anymore, loss of control of torso and legs.” On day nine, “we called the ambulance because we could not get her up.” Once hospitalized, “she was unable to eat or swallow.” Jefferson Healthcare couldn’t stop this downward spiral; my friend’s aunt died in the hospital.
Despite the indisputable temporal relationship to vaccination, despite no other reasonable explanation for her rapid decline and death, and despite the same pattern being seen in significant numbers of elderly around the world post-vaccination—Jefferson County’s doctors, hospital, and health department refused to acknowledge that her “unexpected” demise was caused by the vaccine. Contrary to CDC requirements for healthcare providers, they did not report either the initial adverse event or the death to VAERS, the Vaccine Adverse Events Reporting System.
The cause of death listed on my friend’s aunt’s death certificate was “renal failure”. No mention of the Covid injection that began this cascade of events. A week before her death there had been nothing wrong with her kidneys. Why, after being hospitalized, would they suddenly fail, killing her?
When my friend questioned the attending physician about filing a VAERS report to document an association to the Covid shot, the doctor said she had not reported it. Her rationale was “How can we prove it?”
It is not their job to prove it. The CDC website states:
“Healthcare providers are REQUIRED [their emphasis] to report
to VAERS… adverse events [AEs] after COVID-19 vaccination…
regardless of causality…even if they are not sure if vaccination
caused the event.”
So in a long and difficult process, my friend reported the death to VAERS herself. She then sent a thoughtful email to former health officer Tom Locke, detailing the entire experience with her aunt and Jefferson County’s medical system, cc-ing the doctors involved and several others at Jefferson Healthcare. In her letter, she expressed concern “at the lack of interest in the potential causation or adverse effect the vaccine may have caused.” She noted:
“The instructions for providers giving out any covid shots is they are required to report ANY adverse effect whether or not one can prove causation. As we should all know, these shots are still experimental, hence, the EUA. The very idea that people are racing through drive-thrus to get experimental shots and there seems to be no follow through in reporting adverse or possible adverse effects shows that there is really no scientific methodology happening here. At least at JHC from what I can tell.”
She then described feedback from others she knew who had gotten the shot. Nine out of ten had experienced adverse events—“from extreme pain, aching, headaches, bone infections, diabetic complications, heart decline to death”—and none had been reported to VAERS. Dr. Locke’s response, in part:
“As you correctly note, there does not have to be a proven cause and effect relationship with the observed adverse reactions. Without access to your aunt’s medical records, I am unable to comment on the possible causes of her rapidly progressive illness and death… I think your submission of a VAERS report was the right thing to do. I am not forwarding your note to the Jefferson County Board of Health since investigation of adverse vaccine reactions does not lie within their authority or responsibility.”
In other words, We are going to ignore this.
Our medical professionals at Jefferson Healthcare and the Jefferson County Health Department are out of compliance with CDC requirements. But it is clear that Locke had no intention of correcting the hospital’s failure to report adverse vaccine reactions or to even inform the health board of their lack of compliance. In the campaign to convince everyone to get their shots, public health officials certainly are not going to admit that any county resident was actually harmed, let alone killed by these injections.
Could Jefferson County Public Health’s leadership possibly get worse?
Enter Jefferson County’s new health officer, 36-year-old Dr. Allison Berry. On August 19, 2021, Berry participated in her first official Board of Health meeting. Responding to well-documented Covid vaccine safety issues raised during public comments, she called facts presented “a slurry of outright falsehoods, which is dangerous.” In the inverted narrative being foisted on the public, she herself then spewed what many experts would describe as a stream of misinformation. (See “Health Enforcers Catch Misinformation Fever“)
Insisting that these experimental injections are safe, Berry said with a smile: “There have been no documented deaths due to the Covid-19 vaccine in either of the counties that I oversee.”
Of course there have been no documented deaths here. As with my friend’s aunt, adverse reactions, injuries and fatalities from the shots are being covered up, denied and re-labeled.
Another Jefferson County death directly after the shot that I was alerted to involved a medical practitioner who was instructed to intentionally attribute the death to other causes. “A med provider who lost a patient from injection, was dictated the response required to make,” said an email I received. No surprise that the provider was unwilling to come forward.
There are two consistencies in all the stories you will find here:
1) Vaccine adverse events are rarely, if ever, reported to VAERS.
2) Those talking about these injuries and deaths request anonymity.
Our local heath providers avoid reporting to VAERS to keep the “safe and effective” narrative afloat. Their job is to deny deaths and injuries from the shots, and demonize the healthy unvaccinated to pressure them into “compliance”. Some in our health care system admit privately that this is the narrative they are expected to follow, but they fear losing their jobs if they speak out in public.
Sad testimony to the medical tyranny we have descended into, forbidding transparency… where truth can only be whispered in private.
What is the reality in Jefferson County?
In addition to these deaths, I know two vaxxed people hospitalized for severe clotting, both sent to larger hospitals for treatment, neither acknowledged to be related to their shots. I’ve heard multiple stories about county residents who have been in constant pain since their vaccines, who regret that they succumbed to pressure and media propaganda.
One friend was told by a masked employee at a store checkout that he didn’t want the shot, but got it because he’d been promised he’d be able to work without a mask if he got vaccinated. He was anxious to remove his mask because it gave him severe migraines.
Since his shots, “All of my joints hurt, all of the time,” he said. My friend asked, “Has the pain been getting better over time?” “Not at all,” he said. And now he’s required to mask again, causing him not only to suffer once more from the migraines, but from relentless joint pain from the shots, too. He’s angry—angry enough to complain to a random shopper about the bait-and-switch and about his vaccine injury.
A private healthcare practitioner described a rash of patients coming in post-vax with a range of troubling symptoms. “These symptoms include weeks of unrelenting diarrhea or digestive upset, flares from musculoskeletal conditions like plantar fasciitis, swollen painful joints and nerve pain, headaches and fatigue.”
A doctor told me, “I’ve seen a lot more people having to go to the ER with high blood pressure and atrial fibrillation—enough that they are in danger of having a stroke.” Another contact described a woman who has been having heart issues post-vax. Her heart began racing soon after the shots—tachycardia. She is now on drugs in an effort to keep her heart rate down, with a medical team that doesn’t know what else to do.
An email from a practitioner reported, “A huge proportion of my vaccinated patients had severe side-effects – let’s call them injuries or damage – immediately following vaccination.” Of this large group who experienced injuries, these two gave him permission to be detailed here:
Another local practitioner told me she’d seen four patients with serious adverse effects after their shots. One told her, “I have had a migraine headache ever since I got the vaccine—unrelenting, all day, every day—and the doctors can’t do anything about it.”
The other three, all seen in the same week, had heart emergencies after their shots. One of them, a “perfectly healthy” woman prior to vaccination, had a heart attack. Another had breathing and other lung complications in addition to heart problems. As described below, damage to heart tissue is permanent and is being seen disproportionately in youth receiving the injections. Doctors are concerned that over the next few years many will die from the cardiac stress these vaccine injuries are placing on their hearts.
Among Jefferson Healthcare workers who will not speak publicly for fear of being fired is a hospital employee who in August admitted that HALF of the people they were seeing at the hospital with Covid were fully vaccinated. Data was being manipulated in order to claim that “nearly 90%” of the Covid cases were unvaccinated. (See “Health Enforcers Manipulate Data to Stigmatize Unvaxxed“)
Clotting, blinding headaches, joint pain, bleeding, neurological issues, cognitive impairment, exhaustion and other long-term injuries are being experienced by people who our medical system is at a loss to help. Mental health crises have skyrocketed. And open discussion about this fallout is not allowed.
Two written personal accounts from local residents received:
After a single shot, a second Port Townsend woman wrote, “My symptoms include headache, brain fog, blurred vision, body aches & arthritic pain, and skin sensations like insect bites but nothing there.”
In a follow-up conversation, I learned that she had chosen the J&J vaccine to avoid having to get a second shot. She immediately started experiencing neuropathy, aches all over her body, and extreme fatigue. Her physician prescribed anti-inflammatory medication and she tried numerous detoxes and other interventions. While all these efforts helped some, four months later “none of my issues have totally gone away.”
Just across the inlet on Whidbey Island, a nurse of 35 years shared the denials and cover-ups that are going on there:
“Eight to ten percent of the people I see who got the shots
are very sick or died. Severe reactions—paralysis, heart
issues, miscarriages, clotting, terrible chest pain…”
She has asked many people, “How did you do with the shot?” Some told her they did just fine, didn’t notice any problems. A large number, however, responded, “I regret it. I never felt the same.”
Like Jefferson Healthcare, Whidbey General is short on staff and, therefore, hospital beds. “Staff have all left who don’t want to vaxx,” this nurse said.
The spike protein is a pathogenic toxin – “We made a big mistake.”
In two articles last winter (1) (2), I described mechanisms of damage from these experimental shots that censored doctors and scientists were warning about. Since those articles, even more damning information has come to light.
A bombshell study by researchers at the Salk Institute was published at the end of April showing that the Covid spike protein alone, without the rest of the virus, is a pathogen—toxic. And unlike natural infection which may involve breathing in hundreds or thousands of virus particles, injections directly entering the bloodstream cause the body to produce billions or even trillions of those toxic spike proteins, potentially creating worse damage than contracting Covid naturally.
Dr. Byram Bridle, Associate Professor on Viral Immunology at the University of Guelph in Canada, worked under a government grant to develop a Covid vaccine: He is not only pro-vax, but a vaccine developer. He sounded the alarm in May when he saw the findings of a biodistribution study done by Pfizer. Not released to the public, it was obtained by Japan’s regulatory agency through a freedom of information act request. This research showed that the shot does not remain localized at the injection site as anticipated. Instead, spike proteins are distributed throughout the body, damaging the vascular system, causing strokes, heart inflammation, clotting issues and more.
“We made a big mistake. We never knew the spike protein itself was a toxin and was a pathogenic protein. So by vaccinating people we are inadvertently inoculating them with a toxin… The spike protein gets into the blood, circulates through the blood in individuals over several days post-vaccination. It accumulates in a number of tissues such as the spleen, the bone marrow, the liver, the adrenal glands… in quite high concentrations in the ovaries… it can cross the blood-brain barrier and cause damage to the brain.” [source]
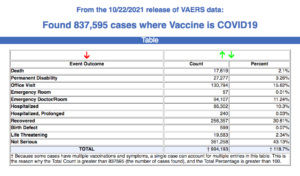
As of October 22, the vastly under-reported VAERS database shows over 800,000 adverse events and 17,619 deaths. That is nearly double all of the reported deaths from every childhood and adult vaccine combined in the 30-year history of VAERS.
A CDC fraud expert says that number of deaths is at least five times, and possibly ten times higher. In July, a whistleblower inside the Centers for Medicare & Medicaid Service (CMS) revealed that their data showed 48,465 people died shortly after receiving their injections. The lawsuit filed against the Department of Health and Human Services which includes the whistleblower’s declaration can be read here.
What have all the autopsies for deaths caused by the Covid shot shown us? As the agency responsible for guaranteeing the safety of this new experimental technology, you’d think that the CDC’s first order of business would be investigating how and why the vaccine was killing people. But the CDC has instead avoided autopsies that would shed light on on post-injection deaths. It took a German scientific report, published in June 2021, to give us the “First case of postmortem study in a patient vaccinated against SARS-CoV-2”.
“Researchers from Germany conducted the world’s first-ever postmortem study on a corpse that had been vaccinated against Covid-19 prior to their death. They discovered that every single organ of the deceased person’s body had become infested with spike proteins as a result of the vaccine.” [source]
Coroners are routinely refusing to conduct autopsies on deaths following Covid vaccination. Cardiologist Dr. Peter McCullough recently lost a patient to the Covid shot. When he ordered an autopsy, the order was denied. Families with loved ones killed by the vaccine are reporting the same experience. One woman’s death less than 24 hours after her first shot was listed as “failure to thrive/heart failure.” Her doctor also requested an autopsy and was refused. So her bereft son paid for one himself. The report confirmed her death was caused by the vaccine.
In a doctors’ roundtable, Dr. Ryan Cole, a pathologist running one of the largest clinical labs in Idaho, noted he was seeing a marked uptick in diseases among the vaccinated: “Post-vaccinated patients are having diseases that we normally don’t see at rates that are considerably alarming.”
Vaccinologist Dr. Robert Malone, one of the inventors of mRNA technology, and a colleague of regulatory agency scientists, confirmed Cole’s observation of disease uptick:
“The FDA is aware of this. This is the kind of thing I find most shocking. The FDA is fully aware that these data exist and yet they’re not disclosing them to the public… Both CDC and FDA are no longer respecting their own rules and laws.”
Out of ethical concerns, Malone, who took the shots himself, has joined the growing number of experts warning that the technology he helped develop is unsafe.
Malone, Bridle, Cole, McCullough, and every other expert exposing this information are under systematic attack by the control system to defame, discredit and silence them.
Now they’re going after the children
Many groups of medical experts around the world are urgently calling for an immediate halt to this experiment, describing it as a crime against humanity. Thousand of doctors and scientists, like Doctors for Covid Ethics, are warning that “Hapless and defenceless children are now becoming victims of the blasphemic and negligently regulated vaccination agenda” (Open Letter and Notice of Liability from Doctors and Scientists). Their scientific papers note that Covid vaccine dangers include “blood clots and leaky vessels,” immunological problems like “enhancing the severity of wild coronavirus infection,” and “flying under the immune system’s radar with the vaccine’s genetic code.”
Still, the pharma/medical/industrial complex presses on, with a constantly-changing narrative designed to stress and confuse, incrementally pushing ever-more oppressive dictates. Now because of the vaccine’s dismal failure to provide any protection at all after only a few months, all the previously “fully vaxxed” need boosters. These boosters will possibly offer a few months of antibodies to the original Covid virus, which is no longer in circulation. It does not protect against Delta or any of the other variants emerging in the vaccinated.
Pressure is ramping up not only to inject all adults, the kids are in the crosshairs. In August, on its Covid-19 webpage, Jefferson County Public Health featured the banner “VAX TO SCHOOL.”
Parroting CDC propaganda, our health department called for children 12 and older—who have statistically zero risk from the virus—to get the shots. The pitch on the website assured us that “COVID-19 vaccines are safe and very effective.”
As illustrated by volumes of data which the industry-captured CDC and FDA are not showing you, both claims are not only false, but inversions of the truth.
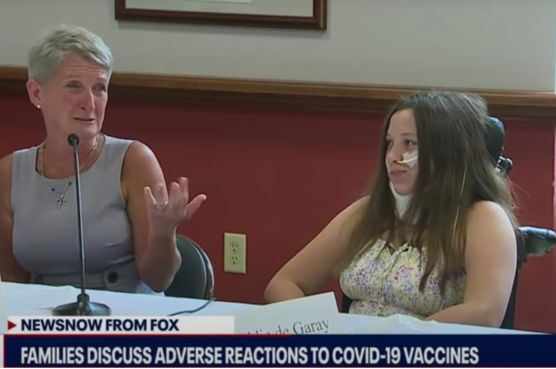
Data disclosed from early Covid vaccine trials on children showed that 85% experienced adverse reactions from mild to serious. Damage from those trials was kept under wraps, as with 12-year-old participant Maddie, whose family took to social media to describe her massive injury. “It has been a frustrating 1.5 months to be told 7 out of the 8 times we took her to the ER, that every test is normal and this is all in her head. Like she can stop the excruciating pain she is in, numbness in her legs and hands, fainting, dizziness, major gastrointestinal issues, fuzzy mind, memory problems, rashes, ulcers and more.”
Maddie, a previously healthy, energetic, straight-A student, was reduced to crippling, scream-inducing pain that landed her in the emergency room within 24 hours of her second Pfizer trial dose. She told her family, “It feels like my heart is being ripped out through my neck.”
Stephanie de Garay testifies about her daughter Maddie’s vaccine injury, June 29, 2021
In a press conference five months later Maddie’s mother, a “pro-vaccine and pro-science” electrical engineer who also volunteered her two sons for the trials, reported:
“Over the next two and a half months her abdominal muscle and nerve pain became unbearable. She developed additional symptoms that included gastroparesis, nausea and vomiting, erratic blood pressure, and heart rate, memory loss; she mixes up words, brain fog, headaches, dizziness, fainting, and then seizures… She developed verbal and motor tics. She had loss of feeling from the waist down and muscle weakness, drastic changes in her vision, urinary retention, and loss of bladder control, severely irregular and heavy menstrual cycles and eventually she had to have an NG tube put in to get nutrition.”
Pfizer tried to cover up the injuries first by calling Maddie a “mental patient,” then denying her problems were related to the vaccine, eventually reporting to the FDA she had “functional abdominal pain” (a stomach ache). Nine months later Maddie is still in a wheelchair, ignored by Pfizer, the FDA, the CDC and the NIH, who are all exempt from liability. [source]
Maddie’s mother asks, “Maddie volunteered for the Pfizer trial, why aren’t they researching her to figure out why this happened so other people don’t have to go through this?… She was totally fine before this. She did the right thing trying to help everybody else and they’re not helping her.”
A mass vaccination event for schoolchildren in Australia—in which parents were denied entry—resulted in at least two children dead, two in comas, and an unknown number of other casualties. In an August 24 interview with Dr. Peter McCullough, he says data from Australia shows that more patients are dying from the vaccine than the virus by 100-fold or more.
Formerly healthy American teens, many of them top athletes, are being hospitalized after the shot for heart damage, and deaths are mounting.
Doctors & Lawyers Issue Dire Warning to High School, College & Pro Athletes
August 8, 2021
On August 8th, medical experts joined sports coaches and an attorney in the webinar “Doctors & Lawyers Issue Dire Warning to High School, College & Pro Athletes.” Top cardiologist Peter McCullough explained (start at 9:07):
“We have about 3,000 certified cases of myocarditis or heart inflammation that have occurred—that’s what the CDC has confirmed. We have no idea how many more thousands of young people have been affected like this. The vaccines all have a dangerous mechanism of action where genetic material is taken up into the heart. It manifests by chest pain, the development of heart failure, EKG changes, abnormal blood tests showing the heart’s being injured, and then it progresses to heart failure or cardiovascular death in some people. I’ve seen these patients in my clinic… It doesn’t look like the vaccine is safe and it doesn’t even look like it works to prevent Covid-19.”
Nuclear cardiologist Dr. Richard Fleming agreed (start at 16:40):
“These viral cardiomyopathies or weakness to the heart, this inflammation and blood clotting occurring with these vaccines, are causing permanent damage to the heart… by and large, once that damage is done, it’s going to be permanent. You’ve got drugs that aren’t having any beneficial effect, but they’re having consequences. The facts in the EUA [Emergency Use Authorization] show these vaccines do not work.”
Former Chief Scientific Advisor to Pfizer, Dr. Michael Yeadon added (start at 34:45):
“All of these products home in to the ovaries and testicles. It’s not benign, it’s going to be harming those tissues. And there’s a second hit—[women’s bodies produce] antibodies against their own placentas when pregnant women are vaccinated with one of these vaccines. It’s just appalling. [There are] also reproductive health risks to males in that they concentrate in testicular tissue. I’m very concerned that they may not be able to have children.”
Putting a final nail in the coffin, pathologist Dr. Ryan Cole described the inability of the current shots to provide any protection at all against prevailing variants (start at 54:25):
“With Delta spreading quickly and being almost 98% of SARS-Cov-2 cases in the US now, this vaccine is out of date, it doesn’t work. The shot does not work against Delta. We’re giving a shot that can do extreme harm to the body, to the brain, to the vesicles, to the heart of these young individuals, and it’s for something that is out of date already.
“You have to realize that more than half of these youth have already had Covid and it is a triple risk for adverse reactions if you give them this shot… to put them at risk for something they don’t need. A broad natural immunity is far better than a vaccine immunity. We know that 17 years later those who have had SARS-Cov-1 still have T-cell memory and immunity. A broad natural immunity is a lifetime immunity.”
As the mainstream narrative about Covid crumbles, we witness increasing desperation to keep the public traumatized and to demonize the Americans who are seeing through the lies. And as more and more people lose faith in our medical system, government and media, pressure continues to ramp up to get dangerous experimental shots in every arm on earth.
It looks like the 5- to 11-year-olds are next
In the May 10 International Journal of Vaccine Theory, Practice, and Research, MIT Senior Research Scientist Stephanie Seneff, PhD, co-authored “Worse Than the Disease?,” an extensive review of unintended consequences from the Covid shots. So disturbed by the science emerging about these vaccines, she has focused her academic research exclusively on this subject over the past year.
Dr. Paul Thomas with MIT scientist Stephanie Seneff, PhD, Episode 020, 10/13/21
Click on image and scroll to breakout interview
In an October 13 interview with pediatrician Dr. Paul Thomas, Seneff describes the effects of “monster messenger RNA” and “neurotoxic spike proteins”:
“The spike protein is neurotoxic… The brain and the heart are really sensitive to this vaccine. This myocarditis [heart inflammation] is really disturbing because the kids are getting a much higher rate of myocarditis… if you’re young you have zero chance of dying from Covid-19. And that vaccine can really mess you up — it can give you permanent heart damage…
“I think the reproductive system could be at great issue here, I think we could be causing a massive infertility crisis in the future generations—especially when we start vaccinating 5-year-old kids. I cannot believe that we’re saying fine, let’s roll it out for the kids… I’m in such a state of shock about this.”
In Sweden, Norway, Finland, and Denmark, Moderna shots have been suspended for young people due to increased risks of heart inflammation. Iceland halted the shots for all ages. Norway opted not to give 12- to 15-year olds second dose shots from any manufacturer because of the incidence of pericarditis and myocarditis, “especially among young men and boys.”
In September 2021, Nobel prize nominee Dr. Vladimir Zelenko co-authored “THE VACCINE DEATH REPORT – Evidence of millions of deaths and serious adverse events resulting from the experimental COVID-19 injections.”
The authors ask, “Why do some people die, or become disabled for life, while others seem just fine after being inoculated?” They point to evidence that “some people get a harmless substance injected, while others get a shot with 5, 10, 20, or 30 micrograms of mRNA… in the booster shots some vials contain as much as 100 or even 250 micrograms of mRNA.”
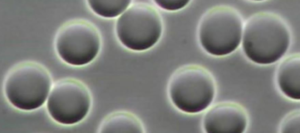
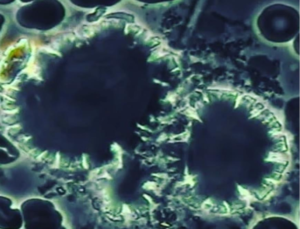
Among the concerns documented in the report are large amounts of graphene oxide found in vaccine vials which can alter our electro-magnetic field and disrupt the normal functioning of organs, permanently altered DNA modifying the human genome, and dramatic damage to blood cells following injection.
Healthy red blood cells are smooth and spherical, non-clumping,
even in color, shape and size.
Micrograph of live blood cells 24 hours after the mRNA vaccine shows crystallized red cells called Heinz bodies, large symplasts of graphene oxide crystals center and Orotic acid crystals in the upper right hand corner.
“We reveal the real risk of an unprecedented genocide… The data suggests that we may currently be witnessing the greatest organized mass murder in the history of our world.”
What if doctors and scientists who are being censored are right?
———————————-
Do you know of local people who have been injured by
(or died from) the Covid injections?
If you have a vaccine injury or death story to share,
please send it to vaxinjury@porttownsendfreepress.com
———————————-
by Craig Durgan | Oct 28, 2021 | General
After declaring a housing emergency in Jefferson County, public officials have now taken action to make the situation worse. On October 4 the Board of County Commissioners declared a new emergency establishing a moratorium on processing housing applications, then on October 11 repealed and replaced it. What’s up with all that?
Our county was already under a housing emergency declared by the BoCC on July 31, 2017 under Resolution 35-17. It has been over 4 years since this declaration, and we still have a dire lack of housing. Even as the BoCC empaneled a task force to “look into it,” we are still lacking housing for both the well-off and those needing affordable housing.
We certainly do not have a lack of land. We do not have a lack of talk. But we do have a lack of action. Let’s look at the talk:
OlyCap talks about constructing an apartment building in Port Townsend next to the Permit center, on land basically donated by Jefferson County. That property acquisition was more than two years ago (September 9, 2019). They even had a ground-breaking ceremony. However, nothing has happened there as yet.
The Legislature allowed some religious organization to install temporary housing on their property. So some “wooden tents” were built. They provide temporary housing to a few.
The County and City engineered the tent camp on the Fairgrounds. That turned out to be a debacle. Now, they have built another tent city on Mill Road.
But aside from these baby steps, the reality has amounted to just talk.
Now the County has declared another housing emergency under Moratorium Ordinance No. 06-1011-21… not to allow more housing, but to prohibit more housing!
That’s right, the County has acted to prohibit housing at the same time as they have a declared housing emergency.
Why have they done this? According to the BoCC’s proclamation, they “enacted a moratorium for one year to pause on certain types of development that could result in densities incompatible with zoning in rural areas.”
But what is meant by incompatible? The minimum lot size in Jefferson County is 5 acres per the zoning regulations. If a lot was in existence prior to the county adopting the Growth Management Act (GMA) it is a legal lot. But now it appears the county might try and make any lot created prior to 1971 unbuildable if it is less than 5 acres.
So the question has to be asked; why is there a 5 acre standard? In the zoning and legal industries it is called a 5 acre bright-line standard.
Under a court case called Thurston County v. W. Wash. Growth Mgmt. Hearings Bd., No. 80115-1, the State Supreme Court ruled that there is no 5 acre minimum “bright-line” standard under the GMA. This was remanded down to the Western Washington Growth Management Board and under Case No. 05-2-0002 Order On Remand Finding Compliance (Rural Lands) stated that:
|
In the Final Decision and Order of July 20, 2005 the Board observed that densities that are no more than one dwelling unit per 5 acres “are generally considered ‘rural’ under the GMA”, and that “Densities that are not urban but are greater than one dwelling unit per 5 acres are generally deemed to promote sprawl in violation of goal 2 of the GMA”, citing numerous prior Board decisions to that effect. In the appeal of this case, the Supreme Court found the application of an urban/rural five acre bright-line exceeded the Board’s jurisdiction. The Board has since followed that Supreme Court directive and will continue to do so.
|
|
In addition, they stated that:
|
The GMA does not define what constitutes “rural densities”; rather, rural densities are “not characterized by urban growth” and are “consistent with rural character.” “Whether a particular density is rural in nature is a question of fact based on the specific circumstances of each case.” Nor does the GMA dictate a specific manner of achieving a variety of rural densities. “Local conditions may be considered and innovative zoning techniques employed to achieve a variety of rural densities.”
|
|
This leaves open the question: What is the minimum lot size in rural lands? To answer this question you need to look at the Growth Management Act:
- Under RCW 36.70A.070(5)(b) it states that: “The rural element shall provide for a variety of rural densities…”
- Under RCW 36.70A.030(17) it states that: “Rural development can consist of a variety of uses and residential densities…”
- Under RCW 36.70A.030(18) it states that: “Rural services do not include storm or sanitary sewers…”
- Under RCW 36.70A.030(20) it states that: “Urban governmental services” or “urban services” include those public services and public facilities at an intensity historically and typically provided in cities, specifically including storm and sanitary sewer systems…”
In other words, the difference between rural and urban is whether there is sewer available or not.
Under WAC 246-272A-0320 Table X the minimum lot size depends on the type of soils and whether there is public water available. The minimum lot size ranges from 12,500 square feet to 2.5 acres.
In considering all the above it is clear that retaining a 5 acre minimum lot size is not consistent with the GMA. In fact, the minimum lot size could be 12,500 square feet (0.2869 acres). It is clearly up to the county to have a range of rural residential densities. Currently the County has not provided a range of rural densities.
Now we get to the crux of this new Emergency Moratorium. There are over 900 subdivisions in Jefferson County. Most of these subdivisions were created prior to 1971. Most of the lots created were less than 12,500 square feet in area.
So some people are trying to use the Boundary Line Adjustment to reconfigure existing lots that are less than 12,500 square feet. Most of the substandard lots (substandard because sewers are not available) are 5,000 to 7,000 square feet.
There are many of these lots in Jefferson County. Once they are reconfigured they can meet the 12,500 square foot minimum to build on septic.
Why should we care? The answer is simple: Under basic economics of supply and demand, as the supply decreases and the demand increase, the price will go up. That is why homes and land are being bid up.
Our supply of homes and land to build on is in short supply, thus the price is going up. This is not a problem for people with the money to bid a home up in value, but it is quite a problem for those of lesser means.
In time this may contribute to areas like Irondale being gentrified… but then where can poorer people there afford to live?
There are many deeply concerned citizens currently working on solutions to our housing crisis. A more democratic approach might have been a concerted effort by county authorities to solicit input from the public prior to instituting a stop-gap measure which, in the near term, is certain to compound the problem.
by Kincaid Gould | Oct 24, 2021 | General
When officials urge the public to “follow the science,” one would think that the appropriate data would be supplied. One would think that asking questions would be allowed. Regrettably, this is far from the case in Jefferson County.
Jefferson County Public Health (JCPH), the Leader and the Peninsula Daily News are the main print sources disseminating COVID-19 information for our county. While the data they publish can provide limited insight into the local COVID situation, there are many aspects of their reporting that are questionable, either because they don’t publish certain data or because they publish misleading data.
For example, data from the Leader indicate that more than half of Jefferson County “COVID deaths” have been in fully vaccinated individuals. That number may be as high as 71%. JCPH’s data also suggests cases among not fully vaccinated individuals outnumber those among fully vaccinated individuals three-to-one. However, this claim relies on misleading data. On the contrary, since early August, more than 40% of Jefferson County cases have been in fully vaccinated individuals. When data is muddled, irrelevant or misrepresented, it is impossible to make sound public health decisions— which, unfortunately, is exactly what Jefferson County Health Officer Allison Berry claims to be doing.
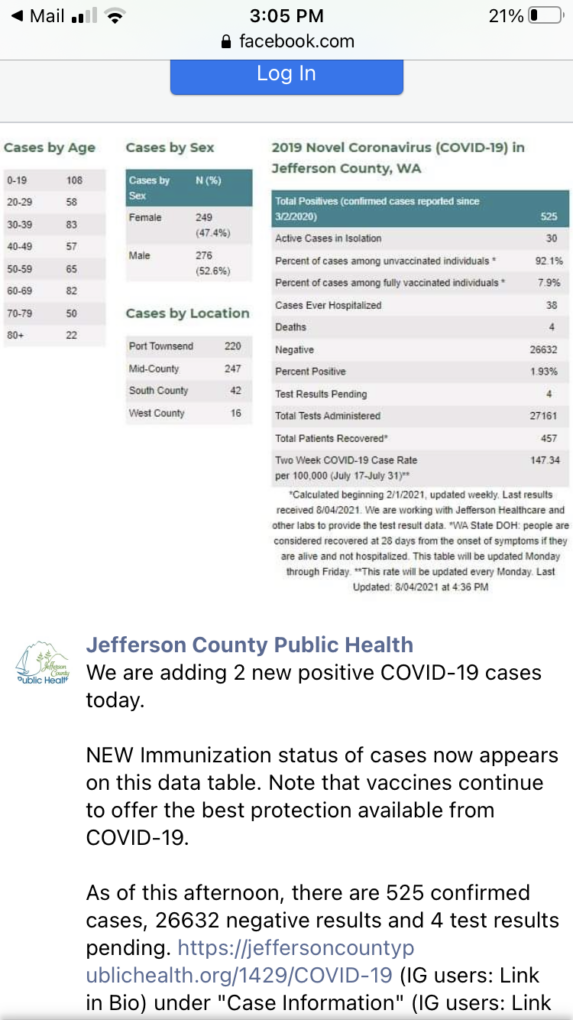
JCPH publishes a daily report with COVID-19 statistics for the county. Recently, I took a look at their data and was struck by the realization that some meaningful data can be extrapolated from some of the misleading statistics they’ve posted. That data, along with some other observations, is presented in the remainder of the article. All data is accurate as of 10/22/2021.
“Fully vaccinated” designation is misleading
The main source of my frustration within JCPH’s data is a pair of statistics (found in the third and fourth rows of the right-most data table): “Percent of cases among (not) fully vaccinated individuals since 2/1/2021.” At first glance, this might seem like an important and informative statistic. After all, this is the clearest data we have locally that informs on whether or not the vaccine actually prevents infection, right? As it turns out, this data is very misleading.
One important aspect to consider is the dichotomy between “fully vaccinated” and “not fully vaccinated”. What exactly do these terms mean? According to the CDC, one isn’t considered “fully vaccinated” until 14 days after they’ve received their last COVID-19 shot — either the single J&J, or the second of the two-dose mRNA jabs. Everybody else is considered “not fully vaccinated,” even if they’ve been “partially vaccinated.”
If all of the shots in a series (and the boosters) are the same, then one would think that being even partially vaccinated would confer some immunity. If being partially vaccinated provides any increase in immunity, there is absolutely no reason why those cases should be included in the same category as individuals who have received no shots.
These two groups seem to be incorrectly interpreted as vaccinated vs unvaccinated by some people—in fact, JCPH was guilty of doing so on 08/04/2021 (see the screenshot). The Peninsula Daily News has run articles that reference these statistics and call the “not fully vaccinated” group “unvaccinated”. While there may be some unvaccinated individuals in the group, it is disingenuous to assume that all of them are. The data provided by JCPH leaves us guessing—it could be a 20-80 split among partially vaccinated and unvaccinated individuals for all we know!
Jefferson County Public Health 8/4/2021 Facebook post
Another problem is that these percentages are measured since 02/01/2021. At this early date, the vast majority of people were not vaccinated, nor were they eligible for vaccination. Most Washington state adults weren’t able to get vaccinated until April 15th, some two and a half months later. Furthermore, if somebody got vaccinated on April 15th and got all of their shots as soon as possible, they wouldn’t be considered “fully vaccinated” until late April (if they chose the J&J shot) or late May (if they received one of the two-dose vaccines).
Why does this matter? Measuring this data from a time when hardly anybody was or could be vaccinated against COVID-19 artificially inflates the number of cases among the “not fully vaccinated’ while decreasing the number among the fully vaccinated. Think about it this way — 0% of COVID-19 cases were found in vaccinated individuals in March 2020. Does this mean that the vaccines are effective? Of course not: the vaccines weren’t available then! Measuring since February 2021 is much better than March 2020, of course, but vaccines were still virtually inaccessible at the start of February.
Speaking of vaccine unavailability, children under the age of 12 are still ineligible for these experimental shots. If the statistics showing the percentage of cases among fully vaccinated and not fully vaccinated individuals is meant to show the vaccine’s efficacy at preventing infection, positive tests among those ineligible for vaccination shouldn’t be included. (I’ll come back to this point later.) Nevertheless, positive tests in this age group are still figured into the data. JCPH lists 151 positive tests among children aged 0-11 since they started collecting data in March 2020. That’s more than one tenth of local cases!
How could this data be improved?
For one, split the data into three categories: fully vaccinated, partially vaccinated, and unvaccinated.
Second, children aged 0-11 should be removed from this specific statistic, as positive tests within this population can’t possibly show the efficacy of the vaccines. This statistic should only include people who are eligible for vaccination at the time when they contract COVID-19. (Previous data should be adjusted to reflect this as well.)
Third, the start date of the data collection should be changed, measuring from May 1st at the very earliest. Better yet, JCPH could publish the percentage of cases among the three groups over a moving time frame. (For example, JCPH publishes a “two-week COVID-19 case rate per 100,000” containing data from the latest two-week period.)
JCPH first published the breakdown of the percentage of positive tests by vaccination status on 08/04/2021 and has updated the statistic at fairly regular intervals ever since. (This data can be found on JCPH’s Facebook page.) Because the percentages among fully vaccinated and not fully vaccinated populations are periodically updated (as is the total number of positive tests), the number of cases among these two populations since 08/04/2021 can be calculated by noting the change in percentages. This data provides a picture of the situation in Jefferson County during just the two-month period from August to October.
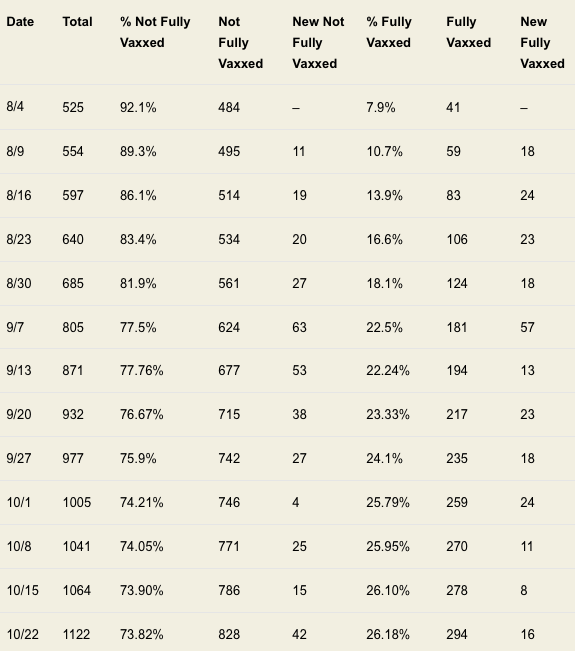
I have created two data tables from JCPH’s updates. The first displays the raw data reported by JCPH, and the total number of cases among the two populations during the period. The second table uses the same information, but removes any cases from before 08/04/2021. Additionally, it presents the percentage of cases added each week in the two groups.
TABLE 1 – Cases Among Not Fully Versus Fully Vaccinated
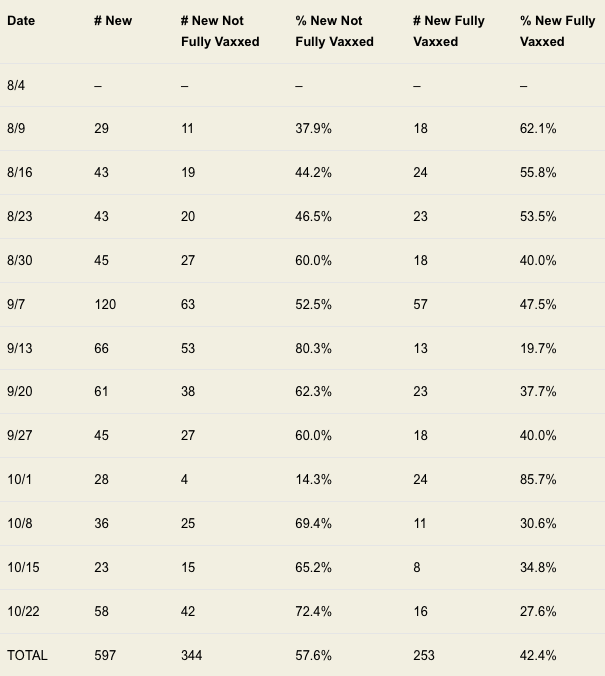
TABLE 2 – New Cases Among Not Fully Versus Fully Vaccinated
There is a clear trend in the percentage share of cases among the two groups since 02/01/2021. As Table 1 shows, the percentage of cases among the not fully vaccinated decreased from 92.1% to 73.82% over the time period, while the percentage among fully vaccinated individuals rose from 7.9% to 26.18%. One possible explanation for this trend is that the data is greatly skewed by the odd start date; this argument is further supported by the fact that even during weeks where there were more cases among not fully vaccinated individuals than among fully vaccinated individuals, the percentage of cases among fully vaccinated individuals increased (for example, during the week of 10/08/2021).
Table 2 makes the data much more clear. Over the period from 08/04/2021 until 10/22/2021, 42.4% of positive tests were among fully vaccinated individuals while 57.6% were from individuals who were either unvaccinated or partially vaccinated. These two percentages are worlds away from the 92.1% and 7.9% rates reported in August. They’re even considerably different from the percentages reported on 10/22/2021 (73.82% vs 26.18%). A 47.64 percentage point difference between 73.82% and 26.18% is more than three times greater than the 15.2 percentage point difference between 57.6% and 42.4%. The differences between these statistics evidently varies greatly with the time frame.
Let’s also consider improper inclusion of ineligible age groups.
On 08/18/2021, JCPH started reporting positive tests with an age band of 0-11-year-olds (replacing an earlier 0-19 age band). As of 8/18/2021, there were 62 individuals in the 0-11 category. By 10/22/2021, there were 151 cases in 0-11-year-olds. Subtracting 62 children from 151, at least 89 individuals aged 0-11 were diagnosed with COVID-19 in the larger period between 08/04/2021 and 10/22/2021. These cases shouldn’t be used to give an idea of vaccine efficacy, as the individuals couldn’t be vaccinated.
Subtracting 89 cases from the “not fully vaccinated” category for the data from 08/04/2021 until 10/22/2021, there are then only 508 total cases, among them 255 cases among the not fully vaccinated population and 253 among the fully vaccinated population. The percentages are virtually identical, with only two more cases found in not fully vaccinated individuals. (Remember that this is a conservative estimate, as there were very likely cases in 0-11-year-olds during the two-week window from 08/04/2021 to 08/18/2021.)
Saying that the vaccine prevents you from catching the virus is misinformation.
The vaccine companies only claim that the vaccine can reduce symptoms, hospitalizations and deaths. Unfortunately, JCPH doesn’t publish the data that could be used to support those claims. The number of asymptomatic and symptomatic cases is not shared (and possibly unknown). The number of fully vaccinated, partially vaccinated and unvaccinated hospitalizations is not reported. Information (e.g., comorbidities, vaccination status, age, date of death, etc.) surrounding alleged COVID-19 deaths is similarly unavailable.
Death data can be extrapolated from articles in the Leader, however, which show that 10 out of 17 ‘COVID’ deaths have been among the fully vaccinated. (Two deaths among the unvaccinated occurred in 2020 and should be discounted when considering vaccine efficacy; a third death reported in mid-April didn’t specify vaccination status. A more accurate number would thus be 10/15 deaths among the fully vaccinated (66.67%), or even 10/14 (71.43%)). It is unclear if the Leader uses the same definition of “unvaccinated” as the Peninsula Daily News (i.e., “not fully vaccinated”) or if it actually means unvaccinated. It is also unclear whether these individuals died of COVID-19 or simply with COVID-19.
If anything, I feel like the points raised above and the data provided by JCPH raise many more questions than they answer. If we are truly in the middle of a dangerous pandemic, shouldn’t the local health department be providing as much relevant and up-to-date information as possible? Are statistics showing the share of males and females who have contracted the virus (which have been divided at around 50-50 since March 2020) really more important than the percentage of deaths and hospitalizations that were among the unvaccinated, partially vaccinated and fully vaccinated?
Keeping information from the public prevents us from “following the science,” and sharing misleading information/pro-vaccine propaganda prevents us from seeing what’s really going on.
by Jim Scarantino | Oct 15, 2021 | General
Local laws can no longer stop religious organizations from hosting the homeless on their property. Tent encampments, tiny homes, safe parking programs, RV living and church buildings used as dormitories and apartments cannot be prohibited by municipal codes or county ordinances.
In 2019 the Washington Legislature enacted a set of laws that explicitly authorize religious organizations to “host the homeless” anywhere on their property, inside or outside buildings. Cities and counties are prohibited from imposing conditions other than those necessary to protect public health and safety. “Necessary” means no less restrictive alternative can be found. Even if “necessary” to serve those goals, the conditions imposed by a city or county may not “substantially burden” the decision of the religious organization regarding the location of a temporary tent encampment, tiny homes village, safe parking program or use of buildings to host the homeless.
The laws are dense, packed with a litany of restrictions on the powers of local government. RCW 35.21.915 applies to most cities and towns. RCW 36.01.290 applies to counties.
This is true separation of church and state. The sovereignty of churches was recognized in medieval times—or so Hollywood tells us in films where the king’s pursuit ends at cathedral doors. Here, in the real world, the legislature has recognized a limited, but still robust sovereignty for church properties.
These laws remain untried and untested in Jefferson County. Earlier in the year the Housing Solutions Network began meeting with churches to encourage hosting programs. Now two churches are going to put the new laws to use. New Life Church Assembly of God in Port Townsend has announced a safe parking program—allowing people to sleep in their cars and RVs. The church already has an RV on its property. The full program, which will accept up to five vehicles to start, is expected to launch mid-November. Another religious organization is on the brink of initiating a safe parking program and I will leave that announcement to them.
These programs would otherwise be illegal under Port Townsend’s prohibition against tent and RV camping. All zoning restrictions are likewise unenforceable against church programs to shelter the homeless.
The tiny home village at the Port Hadlock Community United Methodist Church is not an exercise of that church’s authority to override county ordinances. The quaint village of attractive shelters sits on church property covered by a long-term lease with OlyCap. The project was done in compliance with the county’s regulations, not despite them. That project has motivated other religious organizations to step up and pitch in. I write this article in the hope that it motivates someone to approach their church leadership to consider their own homeless hosting program, be it as modest as providing refuge to just one fellow human being.
In this article I use “churches” and “religious organizations” interchangeably, though the latter term is far broader. The latter term would apply, of course, to a mosque or temple. It also applies to a Unitarian fellowship or Quaker meeting. It would also apply to the home churches scattered around our area, each of which, conceivably, could undertake their own hosting program on residential properties.
This is huge in a small way.
Churches do not need to exhaust the process and bear the cost of obtaining a conditional use permit. All that is required is for the church to hold a public meeting where concerns of neighbors and others may be aired. Then the project may proceed without further ado, even over strenuous objection from neighbors and city officials. (More on that below, under the heading, “Grace.”)
The law, incredibly, puts the burden for providing public notice for the meeting on local government. The religious organization can act quickly, giving the city just 96 hours notice. Then it is up to the city to put out word in newspapers, on its website or via street signs near the meeting place.
The city or county can’t stop the project. It is exempt from all the laws used to delay and frustrate housing development and efforts to shelter the unhoused. There are only a few narrow exceptions, none of which would apply to a safe parking program or tiny home village. Port Townsend’s pre-existing emergency tent encampment rules might apply to a tent encampment, but would not govern RVs on a church property. I also conclude that a church could place mobile homes on its property despite any contrary local regulations.
In the case of a response to a declared emergency, the church can accept homeless on its property without any notice to government or public meeting. The Jefferson County Board of County Commissioners declared a housing emergency in 2017, and reaffirmed that declaration in 2019. That is a sufficient emergency declaration to obviate the legal necessity of scheduling and holding a public meeting. Any church in Jefferson County that takes in someone washed up at their door in need of shelter is on solid footing in immediately letting them pitch a tent, park an RV, move into the church or an outbuilding, or occupy a tiny home.
I think every church should have a foldable cot and inflatable mattress ready in a closet, and, if they have the space, an RV, mobile home and/or tiny home available for such emergencies. “Anyone who sets himself up as ‘religious’ by talking a good game is self-deceived. This is the kind of religion that is hot air, and only hot air. Real religion, the kind that passes muster before God the Father, is this: reach out to the homeless and loveless in their plight, and guard against corruption from a godless world.” 1 James 26-27 (The Message translation).
Constitutional Foundations
This extraordinary development of legislatively carving out refuges from local laws—laws that have contributed greatly to the affordable housing and homelessness crises—is the result of courts’ recognition that serving the homeless is an expression and practice of religious beliefs. The protections of the First Amendment to the United States Constitution and Article I, Section II of the Washington State Constitution operated long before the legislature acted. The right of religious organizations to use their property is actually broader than the statutes in question, which, as the Municipal Research Service Center of Washington has stated, merely attempted to codify and recognize judicial rulings.
The First Amendment right of a church to use its property to care for the homeless was recognized by Congress in the Religious Land Use and Institutionalized Persons Act of 2000 (RLUIP). This law applies the same prohibition against substantially burdening the use of church property. What constitutes “substantial burden”? As explained by the Seattle University School of Law Homeless Rights Advocacy Project: “A substantial burden exists if the religious organization would have to endure additional delay, uncertainty and expense….” Faith is the First Step: Faith-Based Solutions to Homelessness, Means & Rankin (2018).
The rights of a religious organization are even greater under the Washington State Constitution. Washington’s constitution guarantees, “absolute freedom of conscience in all matters of religious sentiment, belief and worship” so long as the practices are not “inconsistent with the peace and safety of the state.” In 2009, in City of Woodinville v. North Shore United Church of Christ, the Washington Supreme Court held that a temporary moratorium on homeless encampments constituted a substantial burden on the church’s religious beliefs and practices and therefore violated the state constitution. The Washington Supreme Court has employed the same “no less restrictive alternative” and “substantial burden” analysis found in the new statutes.
Either We Have An Emergency, or We Don’t
The legislature recognized that we have a dire homelessness crisis, and did not hem or haw about turning religious organizations loose to do something about it.
Churches had encountered one regulatory obstacle after another in seeking to use their property to help the homeless. Winning a lawsuit years down the road was a hollow victory to a church that could barely meet its own overhead, let alone pay for lawyers and legal costs. Very few churches can shoulder the costs of fighting government. And as the cases worked their way through the courts, people in need were denied help.
The legislature disarmed local government, nearly completely.
Zoning and building codes, and enforcement discretion and abuses, are sometimes used to stop projects incrementally instead of issuing an outright permit denial. No more death by a thousand cuts. A city can’t wear down a religious organization by requiring costly insurance. It can’t impose hope-killing time limits or permit fees. It cannot limit the number of homeless being helped, or restrict shelter to only tents, or only RVs or only cars or only tiny homes and then regulate those units to death.
Religious organizations must reasonably comply with fire codes. They must provide portable toilets and wash stations if there is no access to bathrooms. Electrical wiring must, of course, be inspected for safety. The law says that a local government can enact an ordinance requiring a memorandum of understanding (MOU). But the local government can demand very little in the MOU. Mostly it can make recommendations for the religious organization to accept or reject.
Local code enforcement officers and community development directors may not like seeing their powers and discretion nearly cancelled on properties under their jurisdiction. The legislature heard from churches and homeless service agencies about how those powers were being abused to kill their programs. Even if the obstruction was unintentional, merely a routine enforcement of local regulations, the legislature said, “Enough. We have a real emergency. Get out of the way and let religious organizations do what they can to help.”
Grace
Religious organizations would be well advised to show neighbors and city officials the same love and grace they want to show the homeless. Port Townsend residents near churches no doubt fear the prospect of another Fairgrounds encampment disaster. The Fairgrounds tragedy was an example of government neglect and incompetence. Ironically, it was government insistence on onerous, counter-productive regulations that exacerbated the problems. By the city insisting its unrealistically burdensome and costly regulations be enforced, OlyCap, the only agency with the resources to have competently managed the Fairgrounds as an emergency shelter, had to stand back. The Fairgrounds became a Wild West complete with violence, criminality, disease (addiction the most prevalent) and the loss of life.
Religious organizations need to dispel those fears and work closely with local government, service providers and law enforcement to show how to care properly for the homeless. They are not likely to start with the hard cases—the seriously mentally ill and drug addicted. They just don’t have the resources and skills. They are likely going to start with the “easy yesses.” These programs require background checks and are closely coordinated with law enforcement. Social service agencies are engaged to help the churches and the guests. These programs have been very successful elsewhere for many years, with no reports of harm to the surrounding neighborhoods.
Overlake Christian Church in Redmond, for instance, has been hosting young men in its safe parking program. These are individuals early in their working lives who don’t have the cash for “first, last and damage deposit.” By saving up money while they are holding an entry-level job, many have been able to stand on their own feet and move into their first apartment. OCC’s parking program keeps the temporarily homeless from becoming the chronically homeless.
However a church chooses to proceed, it must have a heart for everyone impacted. It is not easy. I have been the point of contact for a campaign by a neighbor of my church who wants a homeless couple moved from where they have set up a stable, healthy home. Their nice RV is separated from the neighbor’s house by a tall, solid fence, and is well over 100 feet from the property line and mostly obscured by an outbuilding. The couple is quiet, tidy and considerate. I find the repeated complaints incomprehensible. I try to see it from the neighbor’s eyes, but can’t. Maybe that comes from growing up in a city of row houses and twins. I just don’t get it.
I strive to respond with courtesy. I pray for compassion and a softening of hearts. I pray for myself that I don’t pridefully stand on the law. But I realize that the law that allows churches to help the homeless is the product of a considered democratic and thorough legislative process. Those bills passed overwhelmingly. Because the homeless may live on church property under the clear terms of the law, they have as much right to eat and sleep where they are as anyone else. I cannot surrender their rights. They would be devastated by the message that they count less than others merely because they have less than others, and that all those professions of love were unreliable. Defending their rights under the law—gracefully—is doing justice.
One Life At A Time Does It
Forget about “ending homelessness.” It’s not going to happen, and there’s nothing a religious organization can do to make it happen. There have always been homeless in this nation. The recent epidemic is, however, truly unprecedented. It has been caused, we are finally learning, not by “the failures of capitalism.” It was capitalism that built apartments and starter homes for generations (and all those affordable row houses in my home town). Exclusionary, aka “snob” zoning and building codes endlessly ratcheting up the cost of construction are the antithesis of free enterprise, by the way.
We have learned that our epidemic of homelessness is caused by the “catastrophic and profound loss of community.” That is the on-the-streets, in-the-trenches observation of the Mobile Loaves and Fishes Ministry of Austin, Texas, the organization behind the ground-breaking and successful Community First! housing development for the chronically homeless.
It is also the conclusion of scholars not beholden to the homelessness-industrial complex, that too often has leveraged the homelessness epidemic for political power and lucrative grants that continue and increase regardless of results. “Homelessness is a condition of disengagement from society–from family, neighborhood, friends, church, and community,” Alice Baum and Donald Burnes wrote in perhaps the definitive book on homelessness. Christopher Rufo, who has produced some excellent documentaries in addition to his scholarly writings, reached the same conclusion, but calls this societal disintegration “disaffiliation.” See my April 20, 2021 article, “Our Fifth Column in the Fight Against Homelessness: Churches.”
This is an opportunity to connect with people who have lost meaningful connection and the sense that they are loved. The genuinely friendly smile delivering a cup of hot coffee to someone who has spent the night in a cold car… you’ve just shown them Jesus without saying a word beyond, “Good morning.”
With the legislature making it clear that little stands in the way of churches employing their resources to shelter the homeless, churches are without excuse in failing to act. It need not be an involved program serving dozens of people, requiring huge expenditures of volunteer time and resources churches may never have unless they accept government funds—a very unwise course for any church. Instead of a grandiose War on Homelessness, it could be as simple as letting a veteran pitch a tent below the stained glass, or a family who have seen their rental sold out from under them using a classroom to keep warm and stay together until they find a new home.
We tend to think in macro terms and set ourselves up for failure and self-recrimination. What difference will it make? The problem is so huge. It is beyond us. We are helpless against such odds.
“There are no great things, only small things done with great love.” That is my favorite quote from Mother Teresa. There is also the starfish story. It has been told many ways. I know this one:
One night a storm washed upon the beach thousands and thousands of starfish. They lay gasping for life on the sand as two men walked along the shore. One started tossing the starfish back into the water, a single dying starfish at a time, He was making no noticeable dent in turning the situation around. “Why bother?” the other man said. “What difference does it make?” His companion bent down to reach a struggling starfish and tossed it back into the sea. “It makes a difference to that one.”
Note to self: Pay attention to the bending down part of the story. That’s important, too.