by Gerald Braude | Jun 26, 2022 | General
Tomorrow, June 27, 2022, Clallam naturopathic physician and author Rick Marschall is due to report for 8 months in jail at the Federal Detention Center in Sheridan, Oregon, after being entrapped in an FDA sting operation. His crime: selling garlic extracts to help COVID-19 patients.
The title of Marschall’s self-published book on Amazon best sums up his philosophy as a naturopathic physician: First Do No Harm. He graduated from Bastyr University in Kenmore, Washington with a license to prescribe anything except opiates. But his focus during his thirty-six years of practice in Clallam County has been on plant-based solutions.
The “Misbranded Drug”: Garlic and Starch
When COVID-19 rolled around, the United States government did not agree with his approach. In the spring of 2020, Marschall says he was having success with a Dynamic Duo product of allicin and larch starch powder for treating this virus.
Allicin is an extract of garlic that serves as an antiviral agent and does not harm good bacteria. The starch, called inuloarabinogalactan (IAG), is a powder from the bark of a larch tree that increases the number of white blood cells available to the immune system.
His book states, “One reason this treatment works so well for COVID-19, a more sophisticated and bioengineered virus, is that this high potency extract of garlic helps to repair damage to the hemoglobin molecule, and it reduces blood clots in the lungs.”
A year later, the National Institute of Health (NIH) confirmed this with an article on its web site. Study results “showed that allicin (L-cysteine) could significantly impact on improvement of signs and symptoms of COVID-19 after two weeks of treatment in comparison to placebo.”
The Sting Operation
Nevertheless, according to court documents, on March 26, 2020, the Food and Drug Administration’s (FDA) Office of Criminal Investigations (OCI) initiated an investigation after receiving complaints “regarding Facebook postings by Marschall and others” about his Dynamic Duo product for treating COVID-19.
On March 30, 2020, an undercover agent for the FDA-OCI texted Marschall that she was “scared about the corona virus so I would like to hear about this product.” The court documents show the two then had a recorded phone conversation in which Marschall said, “Unfortunately, because everybody wants this stuff, you know there’s a bit of a wait.”
The following day, Marshall called and “indicated that the Dynamic Duo was now available.” The undercover agent provided credit card information for the purchase of the product for $140 plus $9.50 for shipping.
On April 2, 2020, by way of the United State Post Office, the product was received in Oakland, California. The undercover agent then mailed the package to the FDA-OCI office in Kirkland, Washington, where they examined the package.
Court documents reveal that the package included a document that stated that the Dynamic Duo “can crush 30 different viral infections, including those in the Corona family, (like in China Corona-19), 40 different bacterial infections, 25 different fungal infections and 20 different parasitic infections like amoebas.”
The special agent concluded in the court document that Marschall “did knowingly and intentionally introduce, deliver, and cause the introduction and delivery for introduction into interstate commerce, drugs, in violation of Title 21, United States Code, Sections 331(a) and 333(a)(2).”
“Because I am a health coach, it would have been okay for me to deliver the product anywhere within state lines,” Marschall said. “My delivery outside of the state would have been okay had I not used a claim or purpose of the product notice. They picked on me to scare people. It doesn’t get any crazier than this.”
The Mistrial
The case was then filed against Marschall in the Federal Western District Court in Tacoma on August 5, 2020. Court documents show he was indicted under 21 U.S.C. 331(a), which prohibits the “introduction or delivery for introduction into interstate commerce of any … drug … that is adulterated or misbranded.”
Marschall said he first received an e-mail from the government and then a letter concerning the case against him. “They could have just sent me a warning letter,” Marschall said. “For example, with a mushroom company that does the same type of thing that I do, the government told them to stop doing it, or else they would shut them down.”
Court document 299 in this case reveals that United States District Court Judge Benjamin H. Settle made the following statement: “While the Food and Drug Administration has discretion to warn or notify individuals or entities it believes are violating FDA regulations, the government is not required to provide individual notice or an opportunity to cease his (Marschall’s) unlawful activity before charging him.”
After a year of proceedings, on August 9, 2021, court documents show that the “jury foreperson declared that the jury is unable to reach a verdict. The jury was polled individually, and all members agree. The Court declares a mistrial.”
After the trial, Marschall says that the judge waived the law shielding jurors from scrutiny and allowed prosecutors to discuss the case with the jurors. As far as Marschall was concerned, this was rare, constitutionally unlawful decision to allow prosecutors to determine the weak points in their case.
Retrial and Conviction
Another trial was carried out in late October. Court documents show that on October 22, 2021 the jury reached the following verdict: “As to the charge of Introduction of Misbranded Drugs into Interstate Commerce, as charged in Count One, we, the Jury, find the Defendant, Richard Marschall guilty.”
Marschall points to the following two injustices during the trial that led to his conviction:
- The judge ordered the jury not to consider any argument relying on the First Amendment’s freedom of speech.
- The judge instructed the jurors not to consider the direct testimony given by a Bastyr University naturopathic professor.
The judge sentenced Marschall to eight months of imprisonment at the Federal Detention Center in Sheridan, Oregon. Judge Settle checked off the following box in his sentencing statement: “The defendant shall surrender for service of sentence at the institution designated by the Bureau of Prisons as notified by the Probation or Pretrial Services Office.”
On May 24, 2022, the judge issued the following: “It is now ordered that the date by which Mr. Marschall must report to FCI Sheridan is extended from May 26, 2022 to no sooner than June 27, 2022.”
Even though this is Marschall’s third conviction in Federal court under the same statute and he had his credential to practice as a naturopathic physician permanently revoked by the state of Washington on October 9, 2018, he remains committed to providing allicin and IAG powder to his COVID-19 patients.
Community Response
Marschall has been active in local health freedom pushback since the lockdowns started, so many friends and well-wishers have been outraged by these injustice proceedings against him. A GiveSendGo campaign was started to help his wife pay bills during his imprisonment.
On June 18, Marschall was lured to the 7th Day Adventist Church in Sequim for a fake “special Vegan Cooking workshop” so the community could instead celebrate him with a surprise 70th birthday party.
Letters of support were sent to the 9th District Court asking for a bond to keep Marschall out of prison. Here’s one from Stephen Schumacher:
Regarding Case# CR20-5270 BHS of the FDA vs. Rick Marschall, please strongly consider expediting a bond to Mr. Marschall so he can stay out of prison until his case is heard on appeal.
As seen in court documents, this is a very troubling case of an undercover sting operation directed against sharing information about a nutritional supplement that anyone can buy on Amazon and has been found to help with Covid-19.
Mr. Marschall is a senior citizen who has caused no harm and is not a danger to anyone; in fact, his supposed crime was trying to help others with treatment options. It is a cruel waste of taxpayer money to incarcerate him prior to appeal.
Please expedite this request before Mr. Marschall must report to FCI Sheridan on June 27.
by Stephen Schumacher | Jun 21, 2022 | General
—————————————–
UPDATE and CORRECTION: After talking this afternoon with Amy Yaley (JHC Director of Marketing and Communications), it appears likely that your medical data is NOT being sent to Facebook through Jefferson Healthcare’s MyChart portal, even though Facebook Pixel Code scripts are present on their regular web pages.
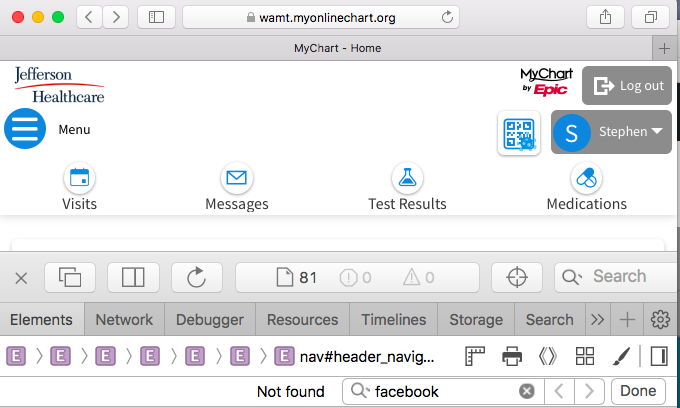
My original article statements were based on recollecting having seen Facebook scripts while inspecting my personal MyChart patient data, but the screenshots below that have evidence of Facebook scripts show the web address “jeffersonhealthcare.org“. If this page had really been from inside MyChart, then the web address would have been “wamt.myonlinechart.org“, as seen in the feature image above.
There are still some unanswered questions, and I am waiting to connect with the person who can answer them. I will update this story with any further clarifications.
What we are left with is that many hospitals around the country have websites that compromise patient data to Facebook, but at this point Jefferson Healthcare does not appear to be one of them.
[Original article text follows:]
Nonprofit technology watchdog The Markup discovered that “a tracking tool installed on many hospitals’ websites (33 of Newsweek’s top 100 hospitals in America) has been collecting patients’ sensitive health information — including details about their medical conditions, prescriptions, and doctor’s appointments — and sending it to Facebook. … We found the tracker, called the Meta Pixel, sending Facebook a packet of data whenever a person clicked a button to schedule a doctor’s appointment.”
This Meta Pixel tracker was detected inside password-protected patient portals such as the MyChart system provided by Jefferson Healthcare. Data breaches uncovered by the crowd-sourced Pixel Hunt project included:
When one real patient who participated in the Pixel Hunt study logged in to the MyChart portal…, the Meta Pixel installed in the portal told Facebook the patient’s name, the name of their doctor, and the time of their upcoming appointment.
When another Pixel Hunt participant used the MyChart portal…, the pixel told Facebook the type of allergic reaction the patient had to a specific medication.
Clicking on one button prompted the pixel to tell Facebook the name and dosage of a medication in our health record, as well as any notes we had entered about the prescription.
Clicking the “Schedule Appointment” button on a doctor’s page prompted the Meta Pixel to send Facebook the text of the button, the name of the doctor, and the search term we used to find the doctor: “Home abortion.”
When The Markup clicked the “Finish Booking” button…, the pixel sent Facebook not just the name of the doctor and her field of medicine but also the first name, last name, email address, phone number, zip code, and city of residence we entered into the booking form.
In addition, if a patient is logged in to Facebook when they visit a hospital’s website where a Meta Pixel is installed, some browsers will attach third-party cookies — another tracking mechanism — that allow Meta to link pixel data to specific Facebook accounts.
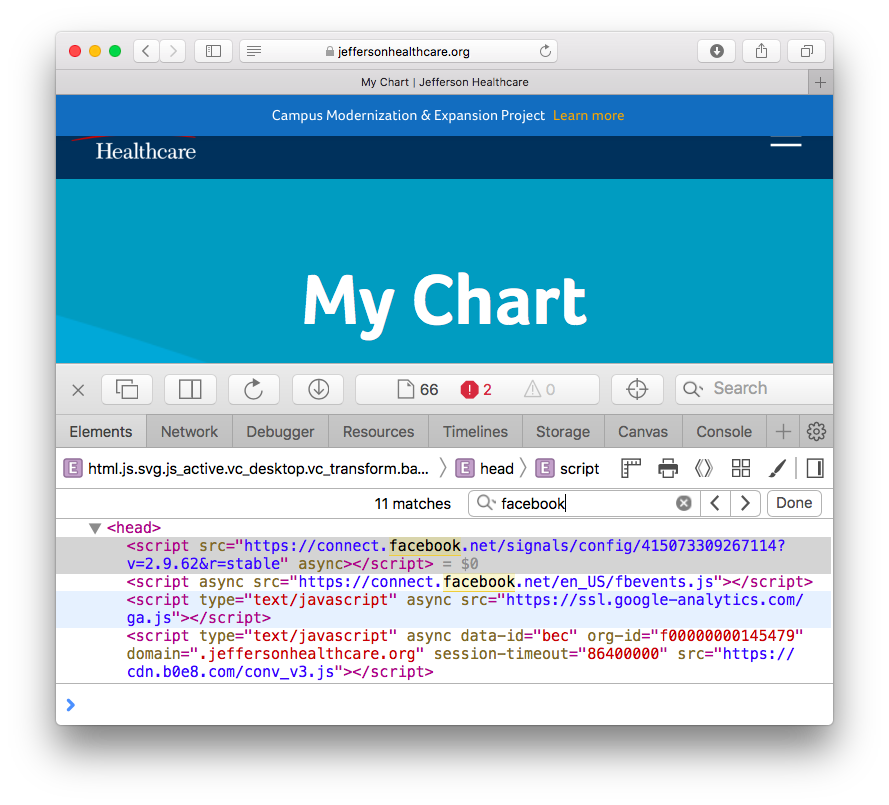
After learning about this potential problem, I signed in to my own Jefferson Healthcare MyChart account, which I’m told “offers secure online access to portions of your electronic health record”. By right-clicking and choosing the “Page Source” or “Inspect” option, it was easy to verify that Jefferson Healthcare’s MyChart webpages are laced with Facebook connections and scripts. See this screenshot:
Here’s another screenshot showing Jefferson Healthcare explicitly including “Facebook Pixel Code” for the Meta Pixel tracking software:
Note that HIPAA law “prohibits covered entities like hospitals from sharing personally identifiable health information with third parties like Facebook, except when an individual has expressly consented in advance or under certain contracts” — which has certainly not happened in this case.
I originally learned about this nationwide problem from Dr. Robert Malone’s substack, where he writes:
I was struck that patients should demand that their data not be entered into such systems. That a movement to return to data entry systems that are not corrupted by Meta, Facebook or Google needs to be jump-started.
As late as 2017, the government was actually worried about medical systems being hacked. But now? Where is our government in protecting patient’s rights?
Clearly, “we” the people can not rely on the US government. Therefore, we have to protect ourselves. Our doctors and hospitals are being encouraged to buy cloud-based, software solutions to “protect us.”
These medical providers also need to be educated — these large cloud systems-based solutions have been corrupted. The medical providers must understand that patients should be given a choice to opt-out of the system. The right to privacy extends to healthcare in its entirety.
The Free Press reached out to Jefferson Healthcare to inform them of this concerning situation and ask for comment. Despite being occupied in an all-day staff meeting at press time, Jefferson Healthcare was able to issue the following statement: “Our goal is to provide exceptional patient care to every patient we serve. Jefferson Healthcare complies with all laws and regulations protecting patient data. We are actively investigating.”
[Editors’ note: The Free Press will update this article as more information becomes available.]
by Stephen Schumacher | Jun 13, 2022 | General
Last June Jefferson County Emergency Management popped up vax clinics at the Saturday Farmers Market, in those pre-booster days excitedly advertising “Johnson & Johnson vaccine available today! One and Done!” Not seeing any takers, I tried talking with one of the masked doctors there, and was surprised by his enthusiasm to give these experimental injections to young children regardless of kids’ risks exceeding benefits for the sake of supposed societal good.
Vaxxers at PT Farmers Market, June 5, 2021 (photo: Stephen Schumacher)
I was reminded of this attitude while reading a peer-reviewed study finding “teenagers are [up to 6 times] more likely to get vaccine-related myocarditis than end up in hospital with Covid,” where a commentator expressed that “Whether or not [young kids] are at high risk relative to the adverse side effects, they should be vaccinated to reduce the probability of older, more at-risk people from getting it.” (Since the injected appear to be more infectious, it’s unclear how that helps grandma.)
This attitude mystified me back then, but I understand it better now after reading Dr. Robert Malone’s explanation of the dark philosophy that has replaced “Do no harm” in modern Public Health:
Dr. Robert Malone interviewed with Dr. Ryan Cole in Gig Harbor, WA on Feb. 21, 2022 (photo: Stephen Schumacher)
As taught in most Universities, “Public Health” (as in the Masters of Public Health degree programs) is also largely based on these two 18th and 19th century philosophical theories (utilitarianism and malthusianism).
As opposed to the disciplines of Medicine and clinical research, which are grounded in the principles of the Hippocratic oath and beneficence as applied to the individual patient.
Examples of beneficence in clinical research and medical practice include “Do no harm,” “Balance benefits against risks,” and “Maximize possible benefits and minimize possible harms.”
What’s so bad about replacing individual patients’ rights and well-being with Public Health’s new utilitarian emphasis on purported “greatest good of the greatest number”? Consider this thought experiment:
A man walks into his doctor’s office for a health checkup. After completion of the exam, he asks “Doc, how am I doing?” His utilitarian MD-MPH turns and says, “You are in perfect health. Your heart is perfect, your liver is perfect, and your kidneys are perfect. And I have four other patients that will die in the next week if they do not get transplants requiring a donated heart, liver or kidney. So I will be prepping you for surgery in one hour.”
Four lives saved for one sacrificed. I think that we can all agree that, while this scenario may meet a utilitarian standard, it fails to meet the fundamentals of Judeo-Christian belief systems regarding the Hippocratic oath and principle of beneficence. But if reports are correct, in the very utilitarian, marxist reality which is modern China under the CCP, organ harvesting is a fact of life.
Dr. Malone concluded that:
As we look back at the long list of public health lies and tragedies that have occurred since January 2020, I have been trying to think through what systemic changes should be implemented to help prevent such catastrophically poor decision making in the future.
I suggest that at the top of the list we include jettisoning both the philosophical dependence of public health decision making (as taught in MPH programs) on utilitarian philosophy, and instead substitute a Judeo-Christian values-based public health decision making process. We have let the MPH utilitarians interject themselves in place of the traditional role of the Physician, and have had to live through the consequences.
Those consequences are now being revealed by research volunteers studying “the 55,000 internal Pfizer documents which the FDA had asked a court to keep under wraps for 75 years”.
PFIZER DOCS: FDA HID PREGNANCY & BABY HARMS
Dr. Naomi Wolf summarized Pfizer documents showing that:
Pfizer (and thus the FDA) knew by December 2020 that the MRNA vaccines did not work — that they “waned in efficacy” and presented “vaccine failure.”
Pfizer knew in May of 2021 that 35 minors’ hearts had been damaged a week after MRNA injection — but the FDA rolled out the EUA for teens a month later anyway, and parents did not get a press release from the US government about heart harms til August of 2021, after thousands of teens were vaccinated.
Athletes and college students and teenagers are collapsing on football and soccer fields. Doctors wring their hands and express mystification. But BioNTech’s SEC filing shows a fact about which the CDC and the AMA breathe not a word: fainting so violently that you may hurt yourself is one of the side effects important enough for BioNTech to highlight to the SEC.
Pfizer (and thus the FDA; many of the documents say “FDA: CONFIDENTIAL” at the lower boundary) knew that … the mRNA spike protein and lipid nanoparticles did not stay in the injection site in the deltoid, but rather went, within 48 hours, into the bloodstream, from there to lodge in the liver, spleen, adrenals, lymph nodes, and, if you are a woman, in the ovaries.
Lipid nanoparticles, the tiny hard fatty casings that contain the MRNA, traverse the amniotic membrane. That means that they enter the fetal environment, of course. (They also traverse the blood-brain barrier, which may help explain the post-MRNA vaccination strokes and cognitive issues we are seeing). … The assurance that the vaccine is “safe and effective” for pregnant women, was based on a study of 44 French rats, followed for 42 days.
While pregnant women were excluded from the internal studies, and thus from the EUA on which basis all pregnant women were assured the vaccine was “safe and effective”, nonetheless about 270 women got pregnant during the study. More than 230 of them were lost somehow to history. But of the 36 pregnant women whose outcomes were followed – 28 lost their babies.
This week the FDA is gearing up to grant new Emergency Use Authorization to inject this witch’s brew into babies as young as 6 months old, and the White House is rolling out 10 million doses prior to authorization.
Biden Administration Makes Available 10 Million Doses of COVID Vaccine for Kids Under 5 — Before FDA Authorizes Shot
Children’s Health Defense chairman Robert F. Kennedy, Jr. gave notice to the FDA and CDC on February 9 and June 10 that:
Should you recommend this pediatric EUA vaccine to children under five years old, CHD is poised to take legal action against you. CHD will seek to hold you accountable for recklessly endangering this population with a product that has little, no, or even negative net efficacy but which may put them, without warning, at risk of many adverse health consequences, including heart damage, stroke and other thrombotic events and reproductive harms.
Commenting on the White House targeting babies with Covid countermeasures that were “never about science or public health” prior to FDA safety review, Kennedy made clear that:
Now they have departed from common sense and into naked cruelty and barbarism. By recommending an unapproved, experimental, zero-liability and high-risk medical intervention for an illness that poses zero statistical danger to that age group, the White House has made itself the enemy of America’s children.
The Pharma gods have demanded child sacrifice and the high priests of public health have offered a generation of infants. Now more than ever, parents and physicians must step into the breach to protect our babies from our government.
Our regulatory agencies and elected officials are not protecting us because they are in lockstep with Big Pharma and mainswamp media promoting this sacrificial message. Their propaganda has been internalized by many who we used to trust to know better, as evidenced by the enthusiasm of the doctor I spoke with at the pop-up vaccine clinic. Jefferson County Public Health’s website is teeming with information on where these dangerous shots are available for 5-11 year olds. Will they soon be adding kids under five?
by Stephen Schumacher | Jun 8, 2022 | General
The Port Townsend City Council opened its June 6 meeting by hearing new police hire Officer Chase Stanton take his Oath of Office.
In public comments, Julie Jaman spoke to the Gateway and Boatyard Expansion Project being hornswoggled by the project mantra “the poplars must go” instead of implementing the Gateway Development Plan that doesn’t envision cutting. Since both PUD and Port have indicated poplars can be worked around, the win-win solution is to remove and replant poplars as needed while pruning suckers per the Plan. Before cutting poplars around town, cost review is needed of functions provided by poplars like unique verticality, buffering, windbraking, storm survivability, filtration, and link to the seasons. Poplars are the right tree in the right place, preventing a paved strip-mall development contrary to community values. *
Harvey Windle focused on problems with the council’s temporary streateries reauthorization until December 31, covering documented damage to business recovery income, lack of notice, not following public input, being out of compliance with state law preventing gifting of public property for these “mess tents”, and aggravating parking scarcity downtown where streateries and all-day parkers make it hard for customers to find places to park.
Stephen Schumacher riffed on Cato’s famous catchphrase by saying “Port Townsend defendenda est” (i.e. PT must be defended), urging the council to stay attentive each meeting to critical police staffing issues, along with getting roads and potholes fixed that were exacerbated by Sunday’s downpour. He reviewed latest findings from The New York Times and elsewhere about masks having infinitesimal effect on Covid spread, their unfitness for purpose since designed for bacteria not aerobic virus transmission, and their many harms especially for kids, so encouraged council to stop modeling their misuse.
City Manager John Mauro responded to public comment by noting council’s wish is to talk about parking management in the next term. Regarding police staffing, the city has just sworn in a new officer, so there is movement in the right direction.
Following staff presentation of interim Ordinance 3291 granting a 6-month extension for temporary tent encampments, pastor Scott Rosenkrans of Port Hadlock Community United Methodist Church spoke of their experience hosting their first Tiny Home encampment. They haven’t had one problem, have enough space for another one, and host a food pantry open Saturdays 10am-1pm, and help folks transition into permanent housing. During the 18 months the tiny homes have been there, they’ve become good neighbors.
Councilor Ben Thomas asked for clarification about the 180 day effective duration of the ordinance and its potential renewal for a second 180 days. City Attorney Heidi Greenwood responded that they’d be vested so eligible for a second extension. Aislinn Diamanti moved, Deputy Mayor Amy Howard seconded, and the council passed the extension unanimously.
After completing some unfinished business adopting Resolution 22-027 for a water system cross connection control program, the council considered Ordinance 3292 to impose a $50 civil infraction for vehicles idling for more than 3 minutes, with exceptions for health or safety reasons, extreme temperatures, traffic stops, law enforcement, vehicle repair, etc.
The proposal arose from the PT High School Students for Sustainability, none of whom were present due to graduation-related conflicts. Attorney Greenwood had helped students with this, and clarified that the exception for health reasons would cover people living in their vehicles.
Thomas wished there was another way to get the same educational result without passing a hard-to-enforce law penalizing idling. Monica MickHager praised the students’ energy, but suggested next time they learn by looking at what codes could be removed to encourage sustainability. Howard felt that if the stated goal is education, then the written warning step shouldn’t be skipped.
Mayor David Faber felt the ordinance should be passed if it’s consistent with our community ideals, but wondered whether officers could be given discretion to issue a warning in lieu of a fine. Heidi explained that generally discretion is always implied on the side of the enforcing officer so long as language “they will” is not there.
After an amusing delay finding a councilor to move the motion, Faber eventually stepped up, Rowe seconded, and the idle ban was passed unanimously.
The council then took up Resolution 22-027 adopting a policy for city fee waivers for intergovernmental cooperation and non-profit organizations that provide community benefits. Howard asked why waivers are limited to two times per calendar year, and Greenwood answered that the intent was to spead them out so they wouldn’t all go to the same organizations. Thomas asked why waivers were limited to non-profits, and Greenwood said this was to keep waivers further from the line where they could be considered gifts of public funds. MickHager moved, Thomas seconded, and the motion carried unanimously.
Next up was Resolution 22-028 to join HUD’s House America initiative to respond with urgency to community homeless crises. Mauro provided background that this came about because councilors Diamanti and Howard sit on the county Housing Fund Board, and staff recommended the city join.
In public comment, Schumacher asked council to evaluate whether anything can be done quickly with the Cherry Street Project to provide housing, and if not, sell it to get this albatross off the books so the money can be used for worthy housing projects. During council deliberation, MickHager wordsmithed characterizing Housing First as “the most effective approach” to “an effective approach”. With that edit, MickHager moved, Diamanti seconded, and the motion carried unanimously.
Concerning the Major’s City Manager Evaluation, MickHager felt he did a good job so moved to approve it, which Diamanti seconded and the council approved unanimously.
In his City Manager’s Report, Mauro started talking about staff comings and going, saying it was great starting a tradition to swear in new police officers before council, feeling that’s right for the duty they provide to our community. That’s a positive, balancing the anticipated resignation of Sgt. Garin Williams after 15 years.
He’s looking to fill other openings, including police, deputy public works directory, and city clerk. Emma Bolin will be joining as Planning Community Development Director, helping among other things with the Evans Vista land purchase.
Mauro spoke of various adventures related to Sunday’s heavy rain downfall, which Public Works responded to quickly. Steve King went on the bluff to look at the stability of the slope, which mostly just lost topsoil… as Mauro quipped, it was interesting to see geology happening in real time.
Mauro feels like Port Townsend is coming back after a couple of years. Rowe was at the previous Farmers Market, and councilors enthusiastically expressed their intent to have one of them appear there the last Saturday of each month to discuss people’s concerns.
Libby Wennstrom asked what our magic number currently is for police staffing. Mauro replied it’s hard to say because we’re now in flux with training. The city has an arrangement with the county as a fallback, but fortunately we haven’t had to call on them and hope to get enough officers to be self-reliant, but as Chief Olson had said, this may take 12-18 months. Other cities are likewise having problems and are down to 30-40% police staffing.
Thomas noted that Windle and others have come to him asking about taking away the temporary streateries; he doesn’t see that happening, but looking at the temporary ordinance, he wonders if they can be terminated if not used for 60 days. Faber mentioned that King had already brought that up with the new owner of Alchemy, whose streatery seems to be rarely used.
Greenwood clarified that the temporary reauthorization until December 31 doesn’t have the same 60 day abandonment clause as in the permanent authorization proposal, but that doesn’t mean the city could not look to exercise it. In terms of process, restaurants don’t have property rights to their allowed streatery slots.
The next regular council meeting on June 20 has been canceled because many members will be out of town that day.
*Correction: The original version inadvertently omitted Julie Jaman’s public comment.
by Kincaid Gould | May 23, 2022 | General
In early December 2021, I submitted a Public Records Request to Jefferson County seeking concrete data on how many COVID-19 cases were in the fully vaccinated, partially vaccinated and unvaccinated categories. In April, I received a redacted spreadsheet containing data from the very first case in March 2020 up until February 24 of this year. The data do not support the claim that the vaccines have had any significant effect on reducing transmission of the Omicron variant locally.
[Note: The spreadsheet that I received was released as a series of images, not a sortable spreadsheet. I have therefore had to count the occurrences of each event by hand. I have made my best effort to get the correct numbers for this article, though it is possible that there was an extra case here or there. If the numbers are not exactly correct, they should be close.]
The most striking feature of this spreadsheet is the column that indicates a person’s vaccination status. The column is filled with a variety of markings indicating how many doses a person had at the time of their symptom onset or their test date.
This specific data was, of course, the most relevant to my question. It is also undoubtedly the data which Public Health Officer Dr. Allison Berry and Jefferson County Public Heath utilize the most frequently to encourage getting vaccinated, saying that the data clearly show that you are more likely to get COVID if you’re unvaccinated.
It was therefore surprising to find that, starting in January (during the relative flood of positive tests reported during the Omicron surge), the vaccination status column becomes only fleetingly filled in. Whereas every cell had something written in it in prior months, there are 498 cases in January 2022 where the vaccination status is simply not listed. That’s a weighty fraction of the 1104 total cases reported that month. It gets even worse in February, with only 104 of the 403 cases having any vaccination information supplied; 299 of the reported cases offer no indication whatsoever.
Note that 797 cases, more than half of the 1507 total cases added to JCPH’s COVID count in January and February, lacked any vaccination status information whatsoever. And yet, to the extent of my knowledge, there has been no mention of this lack of data by Health Officer Berry in the recent months. Not a peep.
Health Officer Berry Zooming into the May 9 BoCC Meeting after learning her daughter tested positive for COVID-19
Public Health appears to be quite comfortable drawing conclusions from a data set missing half of its data. In fact, on January 28, 2022, JCPH stopped reporting the local case rates among the two groups altogether:
“[T]o clarify the impact vaccination status has on COVID-19 case rates… [p]ercentages of cases among the fully and not fully vaccinated in Jefferson County are no longer included on our table.”
Subsequently, the agency started linking to the Washington State Department of Health’s website, which sporadically releases a report on the breakdown of cases in the fully and not fully vaccinated in each county.
At the March 7 Board of County Commissioners meeting, Dr. Berry noted that “state and national numbers do not include antigen tests… all of those case rates at the… state level are only PCRs. That didn’t used to make as big of a difference when very few people were using antigen tests, but in the last month or so, hundreds of millions of antigen tests were pushed out to the public.” She went on to note that antigen tests are counted in Jefferson County, and this is shown in the spreadsheet.
At the April 18 BoCC meeting, the Health Officer said that between 70 and 90 percent of tests reported to JCPH are home antigen tests. During the months of January and February, this rate considerably lower, hanging around 30-40%. At any rate, it’s still a large percentage of the cases. In stopping access to local case rates among the vaccinated and unvaccinated, JCPH has forced us to rely on the state DoH data, which the Health Officer’s assertions suggest may be missing a significant portion of positive antigen tests. How can this be in the public interest or beneficial from a public health standpoint?
But let’s step away from the missing antigen data from the state and refocus on the missing vaccination status data from the county. Despite this gaping hole in the data set, neither Dr. Berry nor JCPH made any comments about a lack in data when positing that Jefferson County was doing “better” than other parts of the state and the country at large because of its high vaccination rate, or that getting vaccinated will lower one’s likelihood of getting COVID. But not only do our local data from that time not support this latter hypothesis; the (known) data actively refute it.
Let’s consider the data from 2022 more closely. If we remove the 797 cases where vaccination status is not listed, we’re left with 710 cases. For purposes of calculating vaccine efficacy, it doesn’t make sense to count cases in children who couldn’t be vaccinated—that would include children 0-4 years old, for whom the vaccine is still not available. There were 26 cases within the time range that had a listed vaccine status—25 unvaccinated, and 1 triple vaccinated, the latter almost certainly a severely immunocompromised child. Removing these 26 children gives a total of 684 cases to work with.
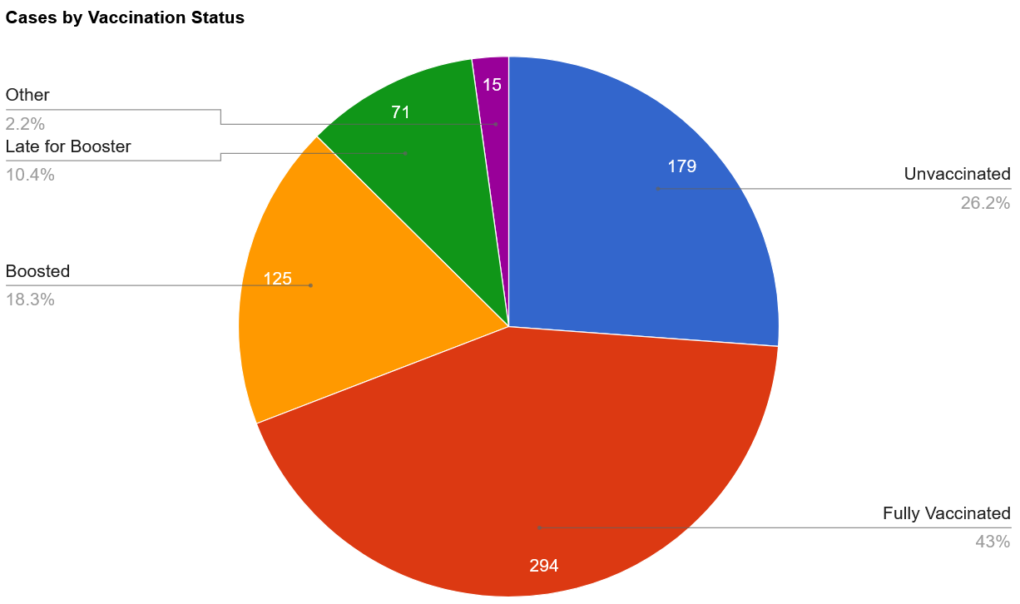
Out of those 684, there were 179 who were clearly labeled as being unvaccinated. 294 were fully vaccinated and were either not due for their booster dose or had no indication that they were late for their booster dose. 125 were boosted. 71 were late for their booster dose or had had their booster dose within 2 weeks prior to their symptom onset. 3 cases in partially vaccinated people (e.g., “1 shot only”) and a smattering of unclear or miscellaneous markings make up the remaining 15 cases, which I’ve placed in the “Other” group in the chart below.
If we translate this into percentages, we have roughly 26.2% of cases in unvaccinated people, 71.6% in those who have received at least two doses of the vaccine, and the remaining 2.2% in people with various miscellaneous statuses.
To determine vaccine efficacy data from this data set alone, the only remaining step is to correct for the relative sizes of the two groups. According to JCPH’s website, 75.8% of the Jefferson County population was fully vaccinated as of February 25, 2022. That means that we would expect 75.8% of the cases to be in the fully vaccinated if the vaccine didn’t reduce one’s chance of catching the virus.
As we can see, the number we’ve come up with (at least 71.6%) is very close to that number, though slightly lower. This suggests that being vaccinated may reduce one’s chance of being infected with Omicron—but if it does, that protection doesn’t seem to be very substantial, as the group accounted for only about 4% fewer cases than would be expected if the vaccine didn’t prevent infection.
Of course, an analysis of this type of data must be taken with a large grain of salt, as there are many confounding factors at play. For one, we know that this data represents fewer than 50% of the total positive tests from January and February. While the scenario is unlikely, if it turned out that all 797 unknown cases occurred in the same group of people, the percentages would significantly shift.
On the other hand, it is feasible (and perhaps even likely) that the distribution of cases in the vaccinated and unvaccinated among the unknown status group would be similar to the distribution among the known status group, so the pie chart above may well be a good indicator of the distribution of cases in Jefferson County. Whatever that distribution is, however, it’s likely to remain unknown. In response to a follow-up email I sent to Public Health asking whether the missing data from the empty cells would be added at a later date, I received a response saying that “No, we have not been able to research vaccination status for past cases.”
We must simultaneously grapple with the fact that the size of each group (vaccinated and unvaccinated) may not be proportional to the size of each group being tested—in other words, it is possible that fewer than 75.8% of the COVID-19 tests are being taken by fully vaccinated people.
For example, if a company requires unvaccinated employees to test weekly for the virus, but has no such requirement for vaccinated workers, this could contribute to an artificial manifestation of a greater case rate in the unvaccinated population simply because they are being tested more often.
The extent to which such procedures are carried out in Jefferson County is not clear, but it is certainly the case in the schools. According to Jefferson County’s “Return to School Flow Chart,” non-fully vaccinated students and staff who have been exposed to COVID-19 must test more frequently than those who have been fully vaccinated. (Note that Port Townsend School District, according to another public records request, was churning out upward of 1000 tests per week in January, and that the other school districts likely had high totals as well.)
The problem of false positives (and negatives) should also be considered. Because a diagnosis by a physician or other medical professional is not necessary to add to the COVID-19 case count in Jefferson County, faulty tests could easily add to the number of cases. If a completely healthy employee is forced to take a test with a 95% accuracy every day, they are expected to churn out a false positive once every 20 days. COVID tests have a variety of accuracy ranges. The possibility of someone having COVID but getting a false negative is also possible.
We also must deal with the nature of the data that’s been collected. Several different people have added information to the spreadsheet, and while there do seem to be some conventions adhered to by most, different people could easily have different tendencies when filling in data. Some entries are much more specific than others, sometimes specifying, for example, the type of vaccine given and its date of administration, while others give only the bare minimum.
Is it possible that somebody, in haste, inputted an entry of “no” in the vaccination status column when the individual was “partially vaccinated”? (When JCPH was still publishing its case rates in the fully vaccinated and not fully vaccinated, partially vaccinated cases were lumped into the latter column together with those who had not received even a single dose of the vaccine.)
Is it possible that someone who was late for the booster did not have that marked down in their cell? There are many different possibilities, and consequently the extent to which these personal choices were applied cannot be puzzled out by simply looking at the table, making it even more difficult to draw solid conclusions.
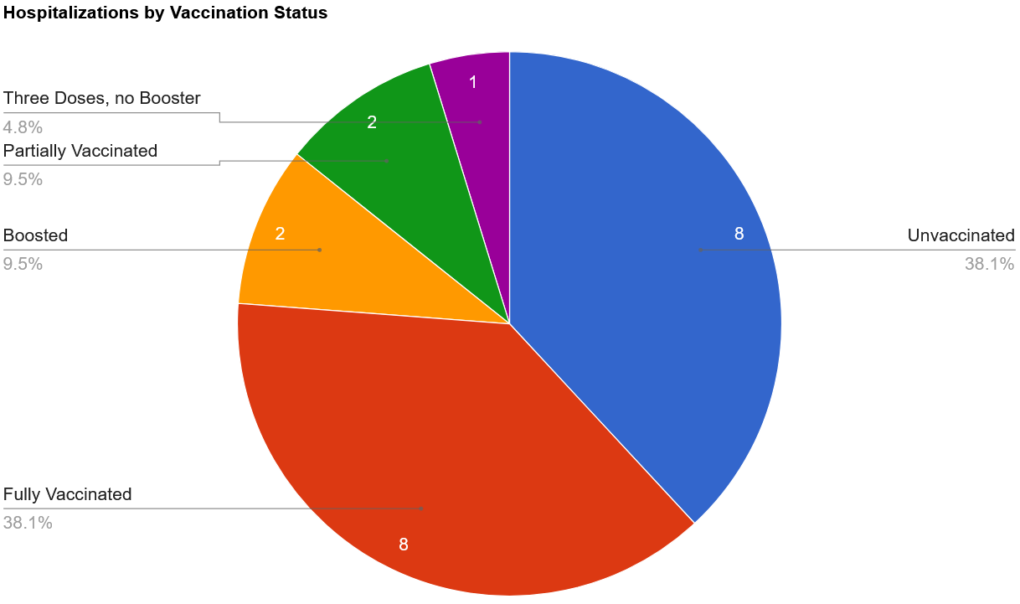
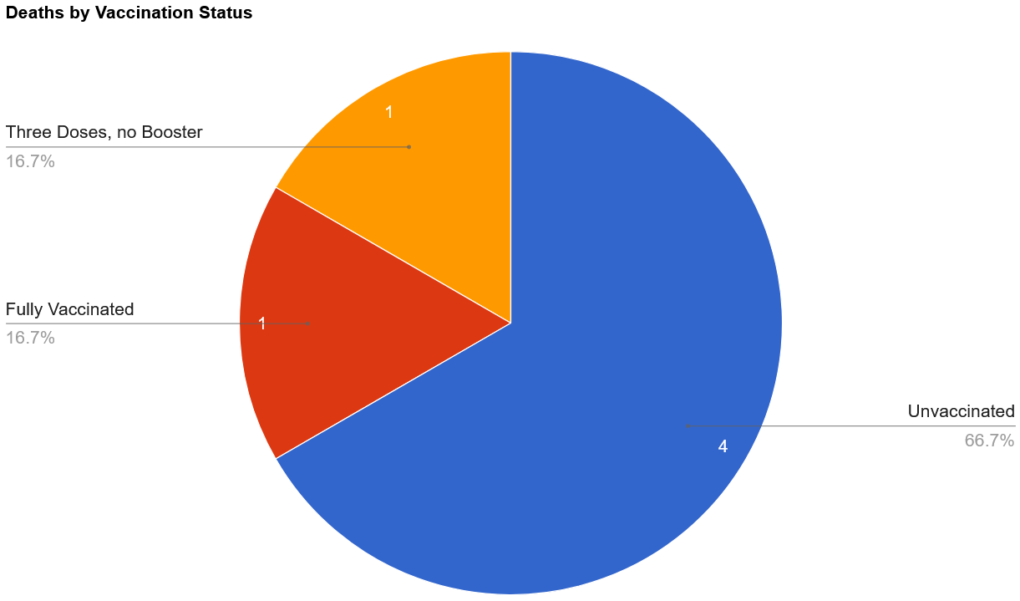
What about hospitalizations and deaths?
There were 27 total hospitalizations in the first two months of the year, with the majority of them (21) occurring in January. In order to hypothesize vaccine efficacy against hospitalization, we are forced to remove 5 of these cases where the vaccine status was left blank. We also should remove the 1 case where the vaccination status was listed as “Not in WAISS,” bringing us down to 21. (WAISS stands for Washington State Immunization Information System, and, according to Public Health, has only been consulted for a small number of cases. Vaccinations that were administered outside of the state or by the military are not recorded in WAISS.)
There were 8 cases in those listed as unvaccinated; 8 in those who were fully vaccinated; 2 in boosted individuals; 2 partially vaccinated, and 1 who had received three doses but was not boosted (likely immunocompromised). Totaling these up, we have 8 cases in the unvaccinated, 2 in the partially vaccinated, and 11 in those who had “completed their primary series.”
There were only 6 deaths, all of them the result of cases that were added to the official count in January. Of those, 2 of them lacked data on vaccination status, 2 were listed as unvaccinated, 1 of them had 3 doses but was not boosted, and 1 was fully vaccinated (no info on booster).
I was surprised to find missing data on vaccination status for hospitalizations and deaths. Hospitalizations and deaths are much more severe outcomes than just having a case of COVID. How could such important data be missing? In response to a query about this disparity, I was told that that vaccination status information likely simply “didn’t get updated on the line list when workloads were very high.” (This is also the reason why there are so many blank cells for cases.) However, even though this data is absent from the spreadsheet, it was reported on in The Leader. Parsing the information shared with The Leader by Public Health with the data in the spreadsheet, it becomes evident that the 2 instances where vaccination status was not listed occurred in unvaccinated individuals.
Interestingly (or perhaps as expected), there’s a theme undercutting all of these deaths. According to The Leader, the first death, a man in his 80s, was unvaccinated and had chronic health conditions.The second death, a woman also in her 80s, was unvaccinated and had chronic medical conditions.The man in his 70s (who had received three doses) was said to have active cancer. The remaining three individuals also all had “chronic medical conditions.” In other words, 100% of the people who died during the Omicron surge (January-February) had chronic medical conditions.
Nevertheless, the percentage of deaths in the unvaccinated (66.7%) is much greater than expected; the percentage of unvaccinated hospitalizations (38.1%) is also quite a bit higher than anticipated. This suggests that the vaccine may have an effect at preventing Omicron-related hospitalizations and deaths.
However, there are confounding factors at play here, as well. One of the most important problems to consider is that we don’t know that any of these individuals actually had the Omicron variant. It’s quite possible that some, or perhaps even all, of them were hospitalized or died with the Delta variant. Recall that all of the deaths occurred in January, closer to when the Delta variant was still the main variant in the community. This is important because the two variants are different in terms of mortality, and a vaccine that protects against one variant isn’t necessarily effective in warding off another.
Regardless of how effective the vaccines were against the Delta variant, there is a general consensus that they are very much less effective against Omicron; in fact, Albert Bourla, CEO of Pfizer, noted in an interview on January 10 that “two doses of a vaccine offer very limited protection, if any” against the Omicron variant. The company is also working on the development of a new vaccine, which wouldn’t be necessary if the current ones were effective against the Omicron variant.
We must also consider the small sample size of the groups. With only 20 hospitalizations (with known vaccination status) and 6 deaths, it is difficult to draw meaningful conclusions. One additional or fewer death could shift the percentages by a considerable amount.
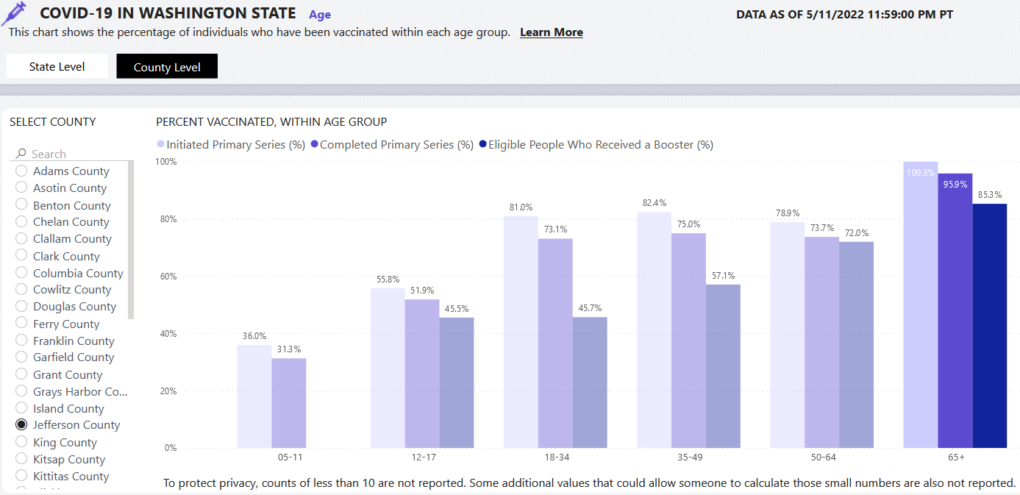
Perhaps even more importantly, we must consider the health of the two groups. Jefferson County is home to a large population of elderly, democratic voters, a group which has shown itself to be very likely to get vaccinated. In fact, if we look at the county-level data on the “Who is getting vaccinated?” tab of the DOH COVID-19 data dashboard, we can see that 100.3% (!) of those over 65 in Jefferson County have at least initiated vaccination. While this is, of course, impossible, and possibly an error resulting from an incorrect population estimate, it does suggest that very few of our county’s seniors are unvaccinated. Indeed, 85.3% of those who were eligible went on to get their booster dose.
Skepticism of the COVID-19 vaccines does not seem to be a thing among the elders of Jefferson County, and so one must ask the question, what might push someone not to get the vaccine? Does the very small number of unvaccinated hospitalization and deaths predominantly include people who had medical contraindications to getting vaccinated? Did a medical professional instruct these people not to get vaccinated because of their condition? When exposed to the virus, would people with chronic medical conditions be more likely to become infected (and thus have to be hospitalized and possibly die) than their healthier counterparts?
Our local Omicron data from January and February point in the direction of a vaccine that is slightly effective at limiting infection, and more effective at preventing hospitalizations and deaths. At the same time, however, there are large holes in the data set that, when filled in, could radically affect how the data could be interpreted. They also present a number of problems intrinsic to the method of data collection and a host of “what if?” questions that seriously hinder drawing any sound conclusions about the efficacy of these injectable products.
While raising more questions than answers, the local data hardly substantiates claims that the vaccines have been effective at preventing infection, hospitalization or death.
by Jim Scarantino | May 19, 2022 | General
Above is a glowing view of San Francisco’s gorgeous Golden Gate Bridge, constructed in under 5 years from 1/5/1933 to 5/28/1937.
What other architectural wonders took less than 5 years to build? A Free Press reader sent us the following list. (Note: The Cherry Street Project is not on this list.)
The Empire State Building, built in 11 months, 3/17/1930-5/1/1931
The Hoover Dam, constructed 4/20/1931-3/1/1936
The Eiffel Tower, constructed 1/1887-3/31/1888
Seattle Space Needle, finished in about 400 days on 4/20/1962
The Pentagon, constructed 9/11/1941-1/14/1943
Disneyland, 1/16/1954-7/17/1955
Transcontinental Canadian Railroad, constructed 1881-1885
The Sears-Willis Tower, built 1970-73
And the tallest building in America since the Sears-Willis Tower was built fast and steadily enough that the Chicago Tribune captured a time-lapse movie of its 2005-2009 construction:
All these marvels got completed in less time than the Cherry Street Project – a rehab of an existing 5,000 sq.ft. building that has been blighting our fair town for 5 years (and counting).
Related: Unhappy Birthday: Cherry Street Project Turns Five Years Old