

In early December 2021, I submitted a Public Records Request to Jefferson County seeking concrete data on how many COVID-19 cases were in the fully vaccinated, partially vaccinated and unvaccinated categories. In April, I received a redacted spreadsheet containing data from the very first case in March 2020 up until February 24 of this year. The data do not support the claim that the vaccines have had any significant effect on reducing transmission of the Omicron variant locally.
[Note: The spreadsheet that I received was released as a series of images, not a sortable spreadsheet. I have therefore had to count the occurrences of each event by hand. I have made my best effort to get the correct numbers for this article, though it is possible that there was an extra case here or there. If the numbers are not exactly correct, they should be close.]
The most striking feature of this spreadsheet is the column that indicates a person’s vaccination status. The column is filled with a variety of markings indicating how many doses a person had at the time of their symptom onset or their test date.
This specific data was, of course, the most relevant to my question. It is also undoubtedly the data which Public Health Officer Dr. Allison Berry and Jefferson County Public Heath utilize the most frequently to encourage getting vaccinated, saying that the data clearly show that you are more likely to get COVID if you’re unvaccinated.
It was therefore surprising to find that, starting in January (during the relative flood of positive tests reported during the Omicron surge), the vaccination status column becomes only fleetingly filled in. Whereas every cell had something written in it in prior months, there are 498 cases in January 2022 where the vaccination status is simply not listed. That’s a weighty fraction of the 1104 total cases reported that month. It gets even worse in February, with only 104 of the 403 cases having any vaccination information supplied; 299 of the reported cases offer no indication whatsoever.
Note that 797 cases, more than half of the 1507 total cases added to JCPH’s COVID count in January and February, lacked any vaccination status information whatsoever. And yet, to the extent of my knowledge, there has been no mention of this lack of data by Health Officer Berry in the recent months. Not a peep.

Health Officer Berry Zooming into the May 9 BoCC Meeting after learning her daughter tested positive for COVID-19
Public Health appears to be quite comfortable drawing conclusions from a data set missing half of its data. In fact, on January 28, 2022, JCPH stopped reporting the local case rates among the two groups altogether:
“[T]o clarify the impact vaccination status has on COVID-19 case rates… [p]ercentages of cases among the fully and not fully vaccinated in Jefferson County are no longer included on our table.”
Subsequently, the agency started linking to the Washington State Department of Health’s website, which sporadically releases a report on the breakdown of cases in the fully and not fully vaccinated in each county.
At the March 7 Board of County Commissioners meeting, Dr. Berry noted that “state and national numbers do not include antigen tests… all of those case rates at the… state level are only PCRs. That didn’t used to make as big of a difference when very few people were using antigen tests, but in the last month or so, hundreds of millions of antigen tests were pushed out to the public.” She went on to note that antigen tests are counted in Jefferson County, and this is shown in the spreadsheet.
At the April 18 BoCC meeting, the Health Officer said that between 70 and 90 percent of tests reported to JCPH are home antigen tests. During the months of January and February, this rate considerably lower, hanging around 30-40%. At any rate, it’s still a large percentage of the cases. In stopping access to local case rates among the vaccinated and unvaccinated, JCPH has forced us to rely on the state DoH data, which the Health Officer’s assertions suggest may be missing a significant portion of positive antigen tests. How can this be in the public interest or beneficial from a public health standpoint?
But let’s step away from the missing antigen data from the state and refocus on the missing vaccination status data from the county. Despite this gaping hole in the data set, neither Dr. Berry nor JCPH made any comments about a lack in data when positing that Jefferson County was doing “better” than other parts of the state and the country at large because of its high vaccination rate, or that getting vaccinated will lower one’s likelihood of getting COVID. But not only do our local data from that time not support this latter hypothesis; the (known) data actively refute it.
Let’s consider the data from 2022 more closely. If we remove the 797 cases where vaccination status is not listed, we’re left with 710 cases. For purposes of calculating vaccine efficacy, it doesn’t make sense to count cases in children who couldn’t be vaccinated—that would include children 0-4 years old, for whom the vaccine is still not available. There were 26 cases within the time range that had a listed vaccine status—25 unvaccinated, and 1 triple vaccinated, the latter almost certainly a severely immunocompromised child. Removing these 26 children gives a total of 684 cases to work with.
Out of those 684, there were 179 who were clearly labeled as being unvaccinated. 294 were fully vaccinated and were either not due for their booster dose or had no indication that they were late for their booster dose. 125 were boosted. 71 were late for their booster dose or had had their booster dose within 2 weeks prior to their symptom onset. 3 cases in partially vaccinated people (e.g., “1 shot only”) and a smattering of unclear or miscellaneous markings make up the remaining 15 cases, which I’ve placed in the “Other” group in the chart below.
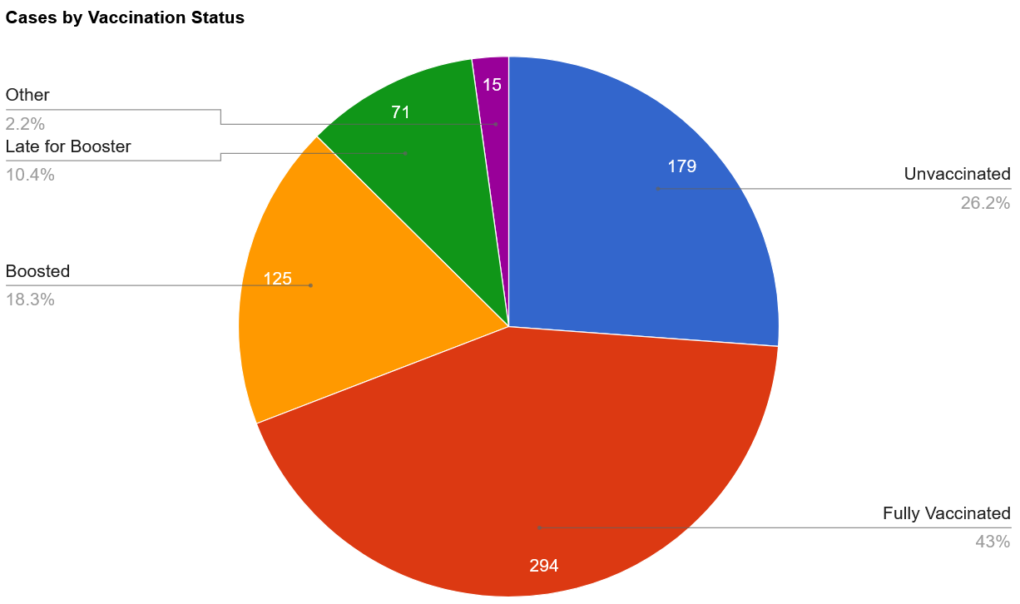
If we translate this into percentages, we have roughly 26.2% of cases in unvaccinated people, 71.6% in those who have received at least two doses of the vaccine, and the remaining 2.2% in people with various miscellaneous statuses.
To determine vaccine efficacy data from this data set alone, the only remaining step is to correct for the relative sizes of the two groups. According to JCPH’s website, 75.8% of the Jefferson County population was fully vaccinated as of February 25, 2022. That means that we would expect 75.8% of the cases to be in the fully vaccinated if the vaccine didn’t reduce one’s chance of catching the virus.
As we can see, the number we’ve come up with (at least 71.6%) is very close to that number, though slightly lower. This suggests that being vaccinated may reduce one’s chance of being infected with Omicron—but if it does, that protection doesn’t seem to be very substantial, as the group accounted for only about 4% fewer cases than would be expected if the vaccine didn’t prevent infection.
Of course, an analysis of this type of data must be taken with a large grain of salt, as there are many confounding factors at play. For one, we know that this data represents fewer than 50% of the total positive tests from January and February. While the scenario is unlikely, if it turned out that all 797 unknown cases occurred in the same group of people, the percentages would significantly shift.
On the other hand, it is feasible (and perhaps even likely) that the distribution of cases in the vaccinated and unvaccinated among the unknown status group would be similar to the distribution among the known status group, so the pie chart above may well be a good indicator of the distribution of cases in Jefferson County. Whatever that distribution is, however, it’s likely to remain unknown. In response to a follow-up email I sent to Public Health asking whether the missing data from the empty cells would be added at a later date, I received a response saying that “No, we have not been able to research vaccination status for past cases.”
We must simultaneously grapple with the fact that the size of each group (vaccinated and unvaccinated) may not be proportional to the size of each group being tested—in other words, it is possible that fewer than 75.8% of the COVID-19 tests are being taken by fully vaccinated people.
For example, if a company requires unvaccinated employees to test weekly for the virus, but has no such requirement for vaccinated workers, this could contribute to an artificial manifestation of a greater case rate in the unvaccinated population simply because they are being tested more often.
The extent to which such procedures are carried out in Jefferson County is not clear, but it is certainly the case in the schools. According to Jefferson County’s “Return to School Flow Chart,” non-fully vaccinated students and staff who have been exposed to COVID-19 must test more frequently than those who have been fully vaccinated. (Note that Port Townsend School District, according to another public records request, was churning out upward of 1000 tests per week in January, and that the other school districts likely had high totals as well.)
The problem of false positives (and negatives) should also be considered. Because a diagnosis by a physician or other medical professional is not necessary to add to the COVID-19 case count in Jefferson County, faulty tests could easily add to the number of cases. If a completely healthy employee is forced to take a test with a 95% accuracy every day, they are expected to churn out a false positive once every 20 days. COVID tests have a variety of accuracy ranges. The possibility of someone having COVID but getting a false negative is also possible.
We also must deal with the nature of the data that’s been collected. Several different people have added information to the spreadsheet, and while there do seem to be some conventions adhered to by most, different people could easily have different tendencies when filling in data. Some entries are much more specific than others, sometimes specifying, for example, the type of vaccine given and its date of administration, while others give only the bare minimum.
Is it possible that somebody, in haste, inputted an entry of “no” in the vaccination status column when the individual was “partially vaccinated”? (When JCPH was still publishing its case rates in the fully vaccinated and not fully vaccinated, partially vaccinated cases were lumped into the latter column together with those who had not received even a single dose of the vaccine.)
Is it possible that someone who was late for the booster did not have that marked down in their cell? There are many different possibilities, and consequently the extent to which these personal choices were applied cannot be puzzled out by simply looking at the table, making it even more difficult to draw solid conclusions.
What about hospitalizations and deaths?
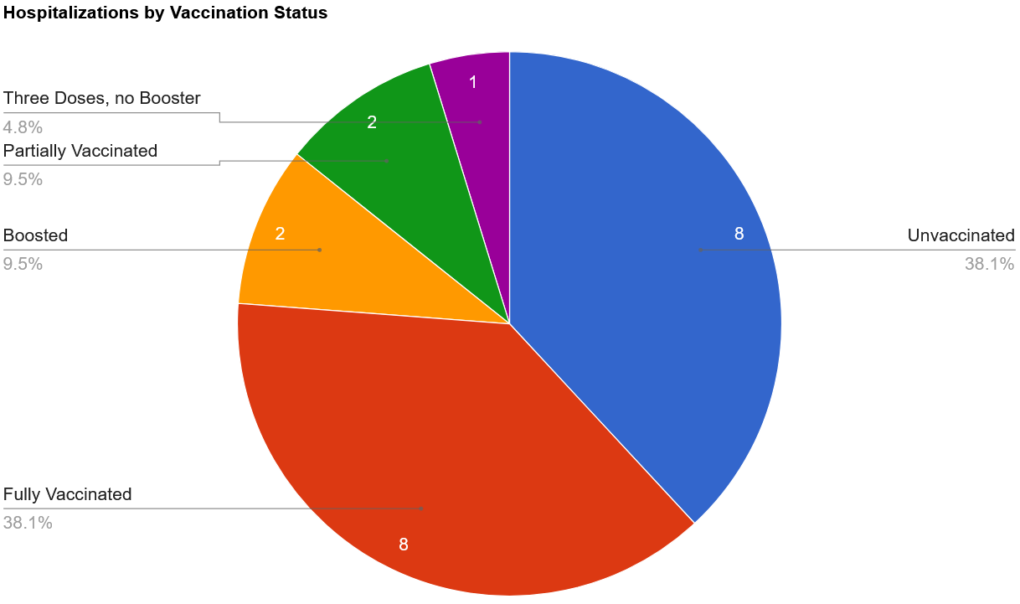
There were 27 total hospitalizations in the first two months of the year, with the majority of them (21) occurring in January. In order to hypothesize vaccine efficacy against hospitalization, we are forced to remove 5 of these cases where the vaccine status was left blank. We also should remove the 1 case where the vaccination status was listed as “Not in WAISS,” bringing us down to 21. (WAISS stands for Washington State Immunization Information System, and, according to Public Health, has only been consulted for a small number of cases. Vaccinations that were administered outside of the state or by the military are not recorded in WAISS.)
There were 8 cases in those listed as unvaccinated; 8 in those who were fully vaccinated; 2 in boosted individuals; 2 partially vaccinated, and 1 who had received three doses but was not boosted (likely immunocompromised). Totaling these up, we have 8 cases in the unvaccinated, 2 in the partially vaccinated, and 11 in those who had “completed their primary series.”
There were only 6 deaths, all of them the result of cases that were added to the official count in January. Of those, 2 of them lacked data on vaccination status, 2 were listed as unvaccinated, 1 of them had 3 doses but was not boosted, and 1 was fully vaccinated (no info on booster).
I was surprised to find missing data on vaccination status for hospitalizations and deaths. Hospitalizations and deaths are much more severe outcomes than just having a case of COVID. How could such important data be missing? In response to a query about this disparity, I was told that that vaccination status information likely simply “didn’t get updated on the line list when workloads were very high.” (This is also the reason why there are so many blank cells for cases.) However, even though this data is absent from the spreadsheet, it was reported on in The Leader. Parsing the information shared with The Leader by Public Health with the data in the spreadsheet, it becomes evident that the 2 instances where vaccination status was not listed occurred in unvaccinated individuals.
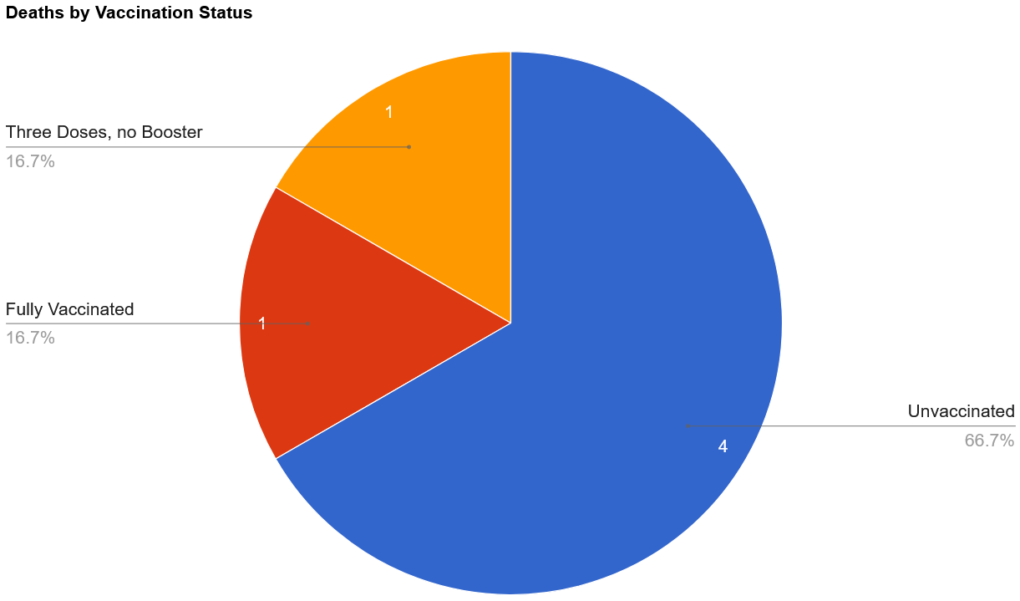
Interestingly (or perhaps as expected), there’s a theme undercutting all of these deaths. According to The Leader, the first death, a man in his 80s, was unvaccinated and had chronic health conditions.The second death, a woman also in her 80s, was unvaccinated and had chronic medical conditions.The man in his 70s (who had received three doses) was said to have active cancer. The remaining three individuals also all had “chronic medical conditions.” In other words, 100% of the people who died during the Omicron surge (January-February) had chronic medical conditions.
Nevertheless, the percentage of deaths in the unvaccinated (66.7%) is much greater than expected; the percentage of unvaccinated hospitalizations (38.1%) is also quite a bit higher than anticipated. This suggests that the vaccine may have an effect at preventing Omicron-related hospitalizations and deaths.
However, there are confounding factors at play here, as well. One of the most important problems to consider is that we don’t know that any of these individuals actually had the Omicron variant. It’s quite possible that some, or perhaps even all, of them were hospitalized or died with the Delta variant. Recall that all of the deaths occurred in January, closer to when the Delta variant was still the main variant in the community. This is important because the two variants are different in terms of mortality, and a vaccine that protects against one variant isn’t necessarily effective in warding off another.
Regardless of how effective the vaccines were against the Delta variant, there is a general consensus that they are very much less effective against Omicron; in fact, Albert Bourla, CEO of Pfizer, noted in an interview on January 10 that “two doses of a vaccine offer very limited protection, if any” against the Omicron variant. The company is also working on the development of a new vaccine, which wouldn’t be necessary if the current ones were effective against the Omicron variant.
We must also consider the small sample size of the groups. With only 20 hospitalizations (with known vaccination status) and 6 deaths, it is difficult to draw meaningful conclusions. One additional or fewer death could shift the percentages by a considerable amount.
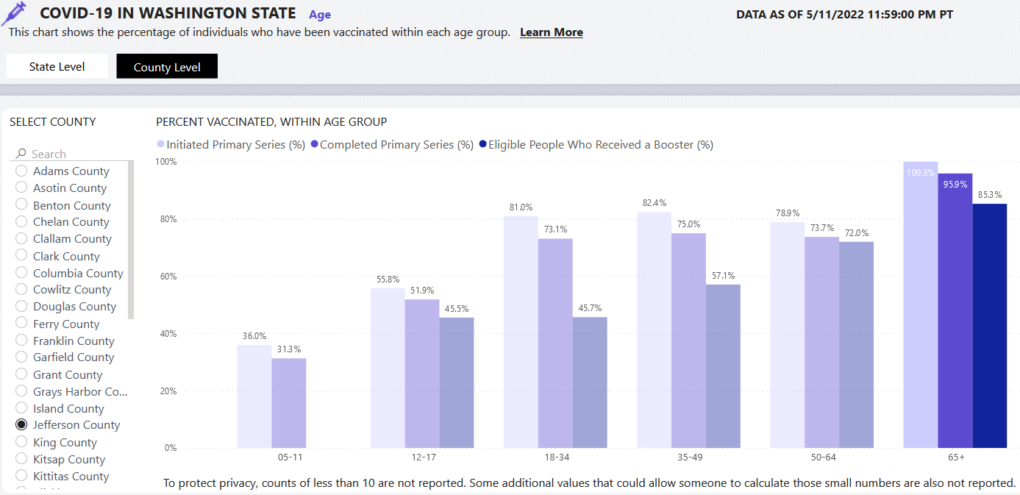
Perhaps even more importantly, we must consider the health of the two groups. Jefferson County is home to a large population of elderly, democratic voters, a group which has shown itself to be very likely to get vaccinated. In fact, if we look at the county-level data on the “Who is getting vaccinated?” tab of the DOH COVID-19 data dashboard, we can see that 100.3% (!) of those over 65 in Jefferson County have at least initiated vaccination. While this is, of course, impossible, and possibly an error resulting from an incorrect population estimate, it does suggest that very few of our county’s seniors are unvaccinated. Indeed, 85.3% of those who were eligible went on to get their booster dose.
Skepticism of the COVID-19 vaccines does not seem to be a thing among the elders of Jefferson County, and so one must ask the question, what might push someone not to get the vaccine? Does the very small number of unvaccinated hospitalization and deaths predominantly include people who had medical contraindications to getting vaccinated? Did a medical professional instruct these people not to get vaccinated because of their condition? When exposed to the virus, would people with chronic medical conditions be more likely to become infected (and thus have to be hospitalized and possibly die) than their healthier counterparts?
Our local Omicron data from January and February point in the direction of a vaccine that is slightly effective at limiting infection, and more effective at preventing hospitalizations and deaths. At the same time, however, there are large holes in the data set that, when filled in, could radically affect how the data could be interpreted. They also present a number of problems intrinsic to the method of data collection and a host of “what if?” questions that seriously hinder drawing any sound conclusions about the efficacy of these injectable products.
While raising more questions than answers, the local data hardly substantiates claims that the vaccines have been effective at preventing infection, hospitalization or death.
Kincaid Gould was born in Port Townsend in 2002. After graduating from Port Townsend High School in 2020, he attended the University of Washington to study music with a focus on the clarinet. Unable to further pursue his studies at UW due to the institution’s (unscientific) COVID-19 vaccination policies, he has returned to Port Townsend, where he enjoys running, cooking, playing music and continuing his education at home.
Regarding home covid 19 antigen tests: turns out the false negative rate may be 20%. The data from Jefferson county relying on self reporting based on a rapid antigen test (lateral flow test) may be inaccurate, meaning the actual case rate may be higher. Here’s an article from the UK. https://www.bmj.com/content/376/bmj-2021-066871
Kincaid, Thank you for good work on the research and article.
My takeaway from your article: There was no data to support the decisions of the Public Health Director and local employers to discriminate against those who choose not to be injected with EUA products.
This data shows minimal if any benefit to the injections. Several other articles on the PTFP show the terrible cost of these injections.
A big “Thank you” to the editors of the PTFP for being a local source of this information.
It seems quite apparent that Berry is clueless, can’t think for herself, swallows the CDC BS hook, line, and sinker, — OR– she is a vindictive sadist who enjoys punishing people because she can. Since she clearly isn’t resigning, we should oust her in the next election if not impeach her before then. She OBVIOUSLY is not doing Jefferson County (or Clallam) any good. What a waste of tax money!
I have not and will not be injected with any of these whatever they are. I believe the research has been rushed too quickly, and certain people have made a lot of money on it. It wasn’t an accident that it started in China. All they had to do is inoculate a group of people and send them around the world to get the results that started this international “”. I have also I ‘am 78 and have been in the Hospital for several things and never tested positive. However, I had four weeks where I’ve wondered if my body took care of me and all of them started about 7pm on a Monday night. The first one I had chills and then elevated temp, but not enough to get up and take a temp. It went away after about two hours. The second week it was back with the same symptoms, it lasted about an hour. The third week nothing. The fourth week is was back and only lasted about half an hour. I think my natural defense took care of it. My blood type isn’t A or O, it’s B-. Also I only wore a mask when the business required it. The reason that was I figured if they got down to fining, I wouldn’t be fined, but the business might be. One last thing. If you want to be protected by a mask, spend the money for a current military mask because that’s the only one you can be sure it will filter just about anything.
Thank you! Good work. I love to see people out in the world thinking critically.
Thank you for a fine article. Strong evidence that musical and mathematical ability go together. I am sure that this entire public health debacle will provide statistics and probability course material for decades.
Thank you for this article Kincaid. Shows the lack of evidence to support such draconian divisive discriminatory mandates. I hope folks can look up from their propaganda news to question what has happened the last two years. Thank you for your hard work.
Medical doctors (Physicians) are supposed to be very scientific; I see very little use of science in any of the decisions of our Public Health Officials.
I am 75 Y.O., I refused any innoculations and wore a mask only when the business required it. I have emphysema, had 3 heart attacks (mild and minmal damge if any), copd.
During the entire “Pandemic” period, I have had 3 bouts of runny nose that lasted 2 to 3 days, used up multiple boxes of “tissue” (kleenex) and have had no other “covid” symptoms. I have not taken a covid test. IMO, this has been a power and money play from the start. The lack of data is probably purposeful so that the actual facts will not come to light and the intentionally (faked) ignorance of most of the (not) “liberal” and many of the republicans can remain intact.
Sad time for America.
Kincaid, and all at PTFP who have endeavored to shed light on the fiasco of local, national, international responses to Covid: Thank you. It is unconscionable that public health policy is based on half-truths, disinformation and outright lies, but welcome to the land of mass-formation psychosis. Coerced and mandated policies centered on public shaming have been our public health officers’ go-to tactic – they’ve marched lockstep with a sociopath (Fauci), without questioning or allowing in any other voices. And our county commissioners sit there, week after week, noses turned up in sanctimony, rolling their eyes at any comments that run counter to their Kool-Aid Narrative. Thank you, PTFP, for pointing out recently that Kate Dean’s “compliant” Portugal, one of the most jabbed nations on earth now boasts one of the highest Covid case rates.
I would like to see data on excess deaths in Jeff and Clallam counties 2020-present. Covid is real, but so is the carnage wrought by lockdowns, vaccine injuries, deaths of despair, poverty, substance abuse.
W.Edward Demings said “In God we trust. All others require data”. John Jamison
Thank you. Fine article. My question (and frustration) is why is natural immunity not addressed?
Linda, how else would make the numbers they come up with if you don’t get to take a shot? It’s all a game of making money by leading the believers to the cool aid, Simple, isn’t it?
One of the most interesting local facets in my parts is how the former “Thurston County manager of COVID data” is now employed as a water quality specialist sending out threat-o-grams on rural Thurstonites’ septic systems. (Both positions paying $56-75K a year [Environmental Health Specialist 2] plus benefits. For nothing more than a college degree, a driver’s license, and “One year of professional environmental health work experience requiring extensive public contact” according to the EHS2 listings on Indeed.)
https://www.zoominfo.com/p/Morgan-Mager/6111543111
https://archive.ph/HxAlz
https://www.thurstoncountywa.gov/tchome/Pages/countynews-detail.aspx?List-ID=54 (put on your AFSCME Karen BrainMelt Protection Helmet before reading that; I read it in Kamala Harris’s voice)
https://archive.ph/emPvf
https://www.thurstoncountywa.gov/phss/Coronavirus/Pages/covid-19-dashboard.aspx
It’s almost as though…I dunno…like…they won’t back down from MUH COVID, coz there might be a chance to harvest state or fed funds later for AAAAAAA about MUH COVID AAAAAAA…but they really don’t have their hearts (careers) in it at the moment.
Of course we know that these county “officials” make a career of posing as experts on all topics…while going from one government sinecure to the next, always with the goal of figuring out the next way to force people to pay for or advance or bow down to their or their handlers’ utopian schemes-of-the-moment. And BOY do they keep coming up with things to intervene in.
https://www.co.thurston.wa.us/health/
https://www.co.thurston.wa.us/health/ehadm/index.html
And to hear them tell it, with the many millions or billions invested in them and their interventions…somehow The Environment (TM) never improves. Which means, of course, we need more of them, not that they’ve failed or whatever.
Meanwhile thousands of hoboes are concentrated in greenspaces/undeveloped pockets in the Olympia area, defecating next to or into waterways, leaving their trash and drugs and needles and garbage everywhere, turning tricks in the parks, dragging their dirty/diseased/unwashed/muddy selves into public and private buildings, dumping lord alone knows what lord alone knows where…
…but somehow it’s dispersed small rural houses and their septic systems that are the big danger to Environmental Health. That and Muh Covid.
The whole thing is such a steaming load of moose doot.
It isn’t possible to thank you enough for the depth of understanding this post represents. We’ve got to shut this system down. It’s NOT democracy, and when enough Americans from all political perspectives actually see it, it’s going to be over
in an instant. Prepare for rough living. Expect to self-rescue. Learn bushcraft. We will beat them. It will take everything we’ve got. I was a liberal when I moved here. Now that I can see what Mainstreet Democrats are actually up to, it’s unlikely I will ever vote for another Democrat again. Certainly not in local politics. This doesn’t mean I don’t care about the planet. It means the planet should be cared for by way of choices made by the American people and no one else. No more McExperts. No more non-profit and NGO grifter “stakeholders”. Enough of their juvenile lingo. Enough of their brainwash marketing buzzwords. ENOUGH!!!
Of the hospitalizations and, in particular, the deaths, how many were hospitalized DUE TO Covid or simply WITH Covid, and how many deaths were FROM Covid rather than simply WITH Covid?