by Kincaid Gould | Oct 30, 2022 | General
BERRY on pharma fraud during vaccine trials:
“[I have been] asked if there have been any valid
concerns raised about Pfizer clinical trials,
about poor design or data falsification…
And the answer is no, actually.”
(2-14-22 BOCC meeting)
FACT CHECK:
Last February, Dr. Berry answered a question about whether or not there was the possibility of fraud in Pfizer’s (still ongoing) clinical trials. “[T]he answer is no, actually,” she said.
According to Dr. Berry, these “were very high quality trials,” and they have been “very heavily scrutinized.” She also pooh-poohed the suggestion that any degree of fraud could have occurred, proclaiming that no “valid concerns… about poor design or data falsification” had been documented.
Enter Brook Jackson
A Certified Clinical Research Professional with almost two decades of experience in a clinical trial setting, Brook Jackson joined Ventavia Research Group in 2020 as a Regional Director. Ventavia had been contracted to carry out clinical research on Pfizer’s vaccine before Jackson signed on, and she began noticing issues as soon as she started work there.
When she brought concerns such as “failure to preserve blinding,” “vaccine dilution errors,” “patient safety issues,” “enrollment and injection of ineligible trial participants,” and “falsification of data” to her supervisors, no actions were taken to remedy the situation. Jackson ultimately related the issues to the FDA, but not without repercussions: just hours after talking with the FDA under supposed confidentiality as a whistleblower, Ventavia contacted Jackson to inform her that she was “not a good fit” for the company and that she was fired.
Brook Jackson was fired from Pfizer contractor Ventavia after bringing safety concerns to the attention of her superiors and the FDA. Watch the BMJ’s 6-minute video of her story.
Refusing to be silenced, Jackson proceeded to file a legal complaint against Ventavia and Pfizer under the False Claims Act (FCA), contending, among other wrongs, that “Pfizer… represented that the clinical trial would comply with all applicable laws and regulations [but that] Defendants violated… multiple FDA regulations when conducting the clinical trial, rendering this certification false.” The 81-page complaint is accompanied by 29 exhibits spanning an additional 551 pages, including emails and text messages, Pfizer source documents, photos of HIPAA and other violations during clinical trials, blood draw data, and lists of errors and deficiencies.
The FCA allows whistleblowers to sue the defendants on behalf and/or with the intervention of the federal government. Suits brought under the FCA are sealed so that the government can investigate the allegations without the defendant’s knowledge. After a period of several months had elapsed with little communication from the government (more on this in a moment), Jackson decided to share her information with the British Medical Journal (BMJ), one of the world’s preeminent and most highly regarded medical publications, despite her case being under seal.
On November 2, 2021, the BMJ published an investigative piece focused on the incident at Ventavia, noting that “Revelations of poor practices at [Ventavia] raise questions about data integrity and regulatory oversight.” The BMJ’s publication enumerates half a dozen specific concerns identified by Jackson:
- Participants placed in a hallway after injection and not being monitored by clinical staff
- Lack of timely follow-up of patients who experienced adverse events
- Protocol deviations not being reported
- Vaccines not being stored at proper temperatures
- Mislabelled laboratory specimens
- Targeting of Ventavia staff for reporting these types of problems.
In its interview with Jackson, the BMJ included a photo Jackson took of a “plastic biohazard bag [that] contained used needles” which should have been disposed of in a sharps box.
(Meta’s fact checker Lead Stories quickly responded by decrying the coverage done by the “British Medical Association’s news blog.” Citing as evidence to rebut the claims of fraud were spokespeople from both Ventavia and Pfizer, the former alleging that “no part of [Jackson’s] responsibilities concerned the clinical trials at issue.”)
Jackson’s case was sealed for more than a year, until early 2022 when the government elected not to intervene in the case. Pfizer filed a motion to dismiss the case in part on the grounds that “the complaint alleges FDA was the victim of ‘fraud’ even though the agency has known about [Jackson’s] allegations for years, has not withdrawn the [vaccine] approvals in question, and continues to express confidence in the data underlying those approvals.” Therefore, even if the court were to find that Pfizer had committed fraud, it wouldn’t matter because the government would have bought their product anyway.
On October 4, the federal government then made a curious move when it submitted a statement of interest supporting Pfizer’s motion to dismiss the case: “[Jackson]’s complaint lacks factual allegations that would support a plausible claim that Ventavia’s clinical trial violations masked problems with the vaccine that were so serious that FDA would have withheld or withdrawn its authorization of the vaccine had it known the truth, such that Pfizer’s subsequent claims for Government payment for the vaccine could be rendered ‘false or fraudulent’ under the FCA.”
Jackson’s attorneys responded on October 27, characterizing the government’s response as an “unusual pleading.” “[T]he government sought this court’s extraordinary seal powers over this case for a substantial time period because of how seriously they took the pleadings as fully legally sufficient as plead…. Had the government truly believed… that [Jackson]’s complaint was devoid of evidence, they would never have required such ample time to investigate.”
Jackson’s attorneys insinuate that if the government was aware of fraud by Pfizer, it could potentially abuse its power to seal the case in order to keep the case out of the public eye — something it succeeded in doing for almost a year before Jackson took her evidence to the BMJ. One can only wonder how many people would have chosen not to take the vaccine if they had known what Jackson knew when she knew it.
As of the publication of this Free Press article, the court has still not ruled on the motion to dismiss.
Jackson’s claims of wrongdoing have received a lot of press, but they aren’t the only reason to suspect fraudulent activity in Pfizer’s clinical trials.
Who is Maddie de Garay?
Earlier this month, Dr. Berry received a simple question: “Who is Maddie de Garay?” In a long-winded response where she not only failed to identify the young teenager by name, but also avoided describing any of the many problems de Garay suffered (and continues to suffer from) immediately after receiving her second Covid-19 shot as part of Pfizer’s clinical trials, Berry also managed to digress from the topic and harp on such things as “right wing talk radio.”
Maddie’s mother, Stephanie de Garay, says that “[i]n less than 24 hours of her second dose, [her previously] healthy and vibrant 12-year-old had a severe systemic adverse reaction.” In her mother’s words, Maddie is now “in a wheelchair, receives all her nutrition and medicine through a feeding tube, cannot control her neck, has constant stomach, back, neck and body pain, vision problems, tinnitus, can’t feel from the waist down, allergic reactions, dysautonomia and… her condition is declining.”
Maddie’s parents have given numerous interviews and even testified on what happened to their daughter (see videos here and here).
Stephanie de Garay testifies on her daughter’s behalf in Washington: “She had severe chest pain. The way she described it, it felt like her ‘heart was being pulled out of her neck.’”
In Pfizer’s report on its trial, there was one participant listed with an ongoing adverse event at the trial cutoff date. Maddie’s adverse events were ongoing when the trial ended, meaning that either the description of that participant, who was “eventually diagnosed with functional abdominal pain,” referred to Maddie, or that Pfizer omitted Maddie from its report to the FDA altogether. Pfizer deemed the adverse event unrelated to the individual’s injections.
Berry sent warm thoughts Maddie’s way over the airwaves noting that she “hope[s] she gets well,” but only after hammering down that “[i]t’s very difficult to say whether or not this girl was even in the trial.” This is an easily contestable claim. Perhaps one of the most convincing pieces of supporting evidence is a recorded phone call between Maddie de Garay’s parents and Dr. Robert Frenck, lead author of the study on the safety of Pfizer’s vaccine in adolescents.
When Dr. Berry then attempted to quash Maddie’s story by suggesting that “it’s just really unclear that those concerns are related to the vaccine,” it became obvious why she had opted not to describe Maddie’s condition in any detail — her paltry ‘lack of causality’ argument is utterly unconvincing and talking about Maddie’s reactions could have potentially fueled local ‘vaccine hesitancy.’
Even if Maddie’s declining physical condition was not a result of vaccination, the situation still merits investigation. To date, this has not occurred, and the de Garay family has been left to pay hundreds of thousands of dollars in medical bills out of pocket. Maddie was one of 1,131 participants in her trial who received the shot, meaning that her extremely severe adverse reaction occurred at a rate of around 884 per million.
Pfizer is accused of fraud not only in the US, but the EU, too.
These are two of the most notable instances of fraud allegations in the context of Pfizer’s Covid-19 shots, but not the only ones.
Concerns have surfaced following the court-ordered release of Pfizer’s clinical trial documents requested under FOIA by Public Health and Medical Professionals for Transparency (PHMPT). A non-profit organization comprised of international scientists and medical experts, PHMPT advocates for data relied upon by the FDA to license Covid-19 vaccines to be publicly available for independent review and analysis. After the FDA attempted to keep the data sealed for 75 years, and Pfizer intervened to also delay its exposure, the court ordered release at a rate of 55,000 pages per month starting on March 1, 2022.
With so much data being released, many eyes have been necessary to pore over the many documents. The FDA has still not yet finished producing all of Pfizer’s data, so it can be difficult to draw certain conclusions until it has released all of its publications.
Just recently, the European Public Prosecutor’s Office announced an investigation into vaccine contracts signed by the EU and Pfizer, opening up the possibility of fraudulent financial activity.
And let’s not forget Pfizer’s track record of paying out multi-million dollar settlements for fraudulent practices (see here, there and everywhere), including what was the largest health care fraud settlement in the history of the US DOJ.
Silencing the alarm and refusing to acknowledge that there even might be fraud going on in Pfizer’s clinical trials as Berry has attempted to do is disingenuous, although perhaps unsurprising given that her incessant exaltation of the vaccines over the past two years has married their two fates together.
———————————-
by Kincaid Gould | May 23, 2022 | General
In early December 2021, I submitted a Public Records Request to Jefferson County seeking concrete data on how many COVID-19 cases were in the fully vaccinated, partially vaccinated and unvaccinated categories. In April, I received a redacted spreadsheet containing data from the very first case in March 2020 up until February 24 of this year. The data do not support the claim that the vaccines have had any significant effect on reducing transmission of the Omicron variant locally.
[Note: The spreadsheet that I received was released as a series of images, not a sortable spreadsheet. I have therefore had to count the occurrences of each event by hand. I have made my best effort to get the correct numbers for this article, though it is possible that there was an extra case here or there. If the numbers are not exactly correct, they should be close.]
The most striking feature of this spreadsheet is the column that indicates a person’s vaccination status. The column is filled with a variety of markings indicating how many doses a person had at the time of their symptom onset or their test date.
This specific data was, of course, the most relevant to my question. It is also undoubtedly the data which Public Health Officer Dr. Allison Berry and Jefferson County Public Heath utilize the most frequently to encourage getting vaccinated, saying that the data clearly show that you are more likely to get COVID if you’re unvaccinated.
It was therefore surprising to find that, starting in January (during the relative flood of positive tests reported during the Omicron surge), the vaccination status column becomes only fleetingly filled in. Whereas every cell had something written in it in prior months, there are 498 cases in January 2022 where the vaccination status is simply not listed. That’s a weighty fraction of the 1104 total cases reported that month. It gets even worse in February, with only 104 of the 403 cases having any vaccination information supplied; 299 of the reported cases offer no indication whatsoever.
Note that 797 cases, more than half of the 1507 total cases added to JCPH’s COVID count in January and February, lacked any vaccination status information whatsoever. And yet, to the extent of my knowledge, there has been no mention of this lack of data by Health Officer Berry in the recent months. Not a peep.
Health Officer Berry Zooming into the May 9 BoCC Meeting after learning her daughter tested positive for COVID-19
Public Health appears to be quite comfortable drawing conclusions from a data set missing half of its data. In fact, on January 28, 2022, JCPH stopped reporting the local case rates among the two groups altogether:
“[T]o clarify the impact vaccination status has on COVID-19 case rates… [p]ercentages of cases among the fully and not fully vaccinated in Jefferson County are no longer included on our table.”
Subsequently, the agency started linking to the Washington State Department of Health’s website, which sporadically releases a report on the breakdown of cases in the fully and not fully vaccinated in each county.
At the March 7 Board of County Commissioners meeting, Dr. Berry noted that “state and national numbers do not include antigen tests… all of those case rates at the… state level are only PCRs. That didn’t used to make as big of a difference when very few people were using antigen tests, but in the last month or so, hundreds of millions of antigen tests were pushed out to the public.” She went on to note that antigen tests are counted in Jefferson County, and this is shown in the spreadsheet.
At the April 18 BoCC meeting, the Health Officer said that between 70 and 90 percent of tests reported to JCPH are home antigen tests. During the months of January and February, this rate considerably lower, hanging around 30-40%. At any rate, it’s still a large percentage of the cases. In stopping access to local case rates among the vaccinated and unvaccinated, JCPH has forced us to rely on the state DoH data, which the Health Officer’s assertions suggest may be missing a significant portion of positive antigen tests. How can this be in the public interest or beneficial from a public health standpoint?
But let’s step away from the missing antigen data from the state and refocus on the missing vaccination status data from the county. Despite this gaping hole in the data set, neither Dr. Berry nor JCPH made any comments about a lack in data when positing that Jefferson County was doing “better” than other parts of the state and the country at large because of its high vaccination rate, or that getting vaccinated will lower one’s likelihood of getting COVID. But not only do our local data from that time not support this latter hypothesis; the (known) data actively refute it.
Let’s consider the data from 2022 more closely. If we remove the 797 cases where vaccination status is not listed, we’re left with 710 cases. For purposes of calculating vaccine efficacy, it doesn’t make sense to count cases in children who couldn’t be vaccinated—that would include children 0-4 years old, for whom the vaccine is still not available. There were 26 cases within the time range that had a listed vaccine status—25 unvaccinated, and 1 triple vaccinated, the latter almost certainly a severely immunocompromised child. Removing these 26 children gives a total of 684 cases to work with.
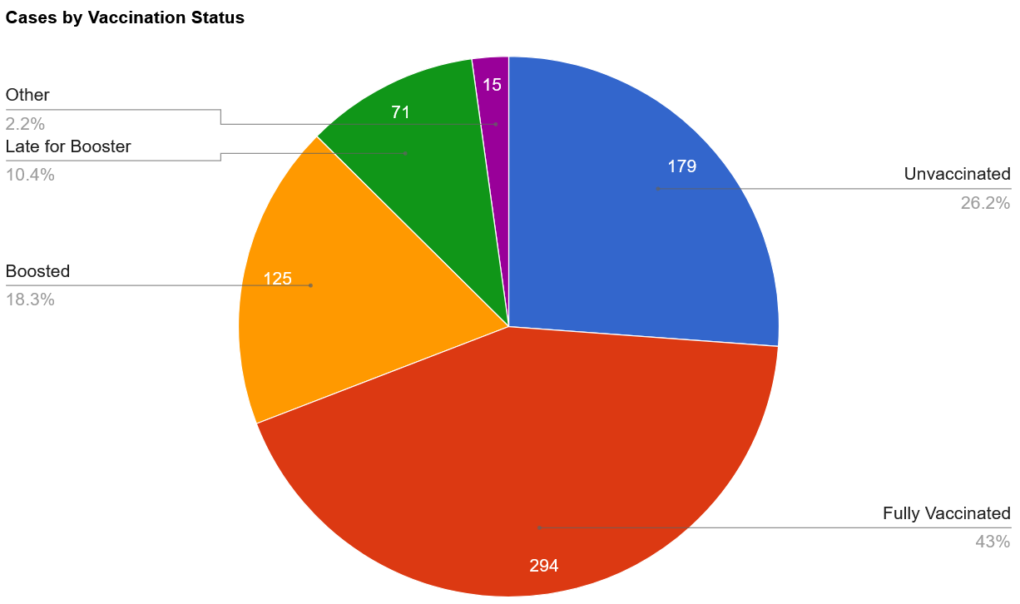
Out of those 684, there were 179 who were clearly labeled as being unvaccinated. 294 were fully vaccinated and were either not due for their booster dose or had no indication that they were late for their booster dose. 125 were boosted. 71 were late for their booster dose or had had their booster dose within 2 weeks prior to their symptom onset. 3 cases in partially vaccinated people (e.g., “1 shot only”) and a smattering of unclear or miscellaneous markings make up the remaining 15 cases, which I’ve placed in the “Other” group in the chart below.
If we translate this into percentages, we have roughly 26.2% of cases in unvaccinated people, 71.6% in those who have received at least two doses of the vaccine, and the remaining 2.2% in people with various miscellaneous statuses.
To determine vaccine efficacy data from this data set alone, the only remaining step is to correct for the relative sizes of the two groups. According to JCPH’s website, 75.8% of the Jefferson County population was fully vaccinated as of February 25, 2022. That means that we would expect 75.8% of the cases to be in the fully vaccinated if the vaccine didn’t reduce one’s chance of catching the virus.
As we can see, the number we’ve come up with (at least 71.6%) is very close to that number, though slightly lower. This suggests that being vaccinated may reduce one’s chance of being infected with Omicron—but if it does, that protection doesn’t seem to be very substantial, as the group accounted for only about 4% fewer cases than would be expected if the vaccine didn’t prevent infection.
Of course, an analysis of this type of data must be taken with a large grain of salt, as there are many confounding factors at play. For one, we know that this data represents fewer than 50% of the total positive tests from January and February. While the scenario is unlikely, if it turned out that all 797 unknown cases occurred in the same group of people, the percentages would significantly shift.
On the other hand, it is feasible (and perhaps even likely) that the distribution of cases in the vaccinated and unvaccinated among the unknown status group would be similar to the distribution among the known status group, so the pie chart above may well be a good indicator of the distribution of cases in Jefferson County. Whatever that distribution is, however, it’s likely to remain unknown. In response to a follow-up email I sent to Public Health asking whether the missing data from the empty cells would be added at a later date, I received a response saying that “No, we have not been able to research vaccination status for past cases.”
We must simultaneously grapple with the fact that the size of each group (vaccinated and unvaccinated) may not be proportional to the size of each group being tested—in other words, it is possible that fewer than 75.8% of the COVID-19 tests are being taken by fully vaccinated people.
For example, if a company requires unvaccinated employees to test weekly for the virus, but has no such requirement for vaccinated workers, this could contribute to an artificial manifestation of a greater case rate in the unvaccinated population simply because they are being tested more often.
The extent to which such procedures are carried out in Jefferson County is not clear, but it is certainly the case in the schools. According to Jefferson County’s “Return to School Flow Chart,” non-fully vaccinated students and staff who have been exposed to COVID-19 must test more frequently than those who have been fully vaccinated. (Note that Port Townsend School District, according to another public records request, was churning out upward of 1000 tests per week in January, and that the other school districts likely had high totals as well.)
The problem of false positives (and negatives) should also be considered. Because a diagnosis by a physician or other medical professional is not necessary to add to the COVID-19 case count in Jefferson County, faulty tests could easily add to the number of cases. If a completely healthy employee is forced to take a test with a 95% accuracy every day, they are expected to churn out a false positive once every 20 days. COVID tests have a variety of accuracy ranges. The possibility of someone having COVID but getting a false negative is also possible.
We also must deal with the nature of the data that’s been collected. Several different people have added information to the spreadsheet, and while there do seem to be some conventions adhered to by most, different people could easily have different tendencies when filling in data. Some entries are much more specific than others, sometimes specifying, for example, the type of vaccine given and its date of administration, while others give only the bare minimum.
Is it possible that somebody, in haste, inputted an entry of “no” in the vaccination status column when the individual was “partially vaccinated”? (When JCPH was still publishing its case rates in the fully vaccinated and not fully vaccinated, partially vaccinated cases were lumped into the latter column together with those who had not received even a single dose of the vaccine.)
Is it possible that someone who was late for the booster did not have that marked down in their cell? There are many different possibilities, and consequently the extent to which these personal choices were applied cannot be puzzled out by simply looking at the table, making it even more difficult to draw solid conclusions.
What about hospitalizations and deaths?
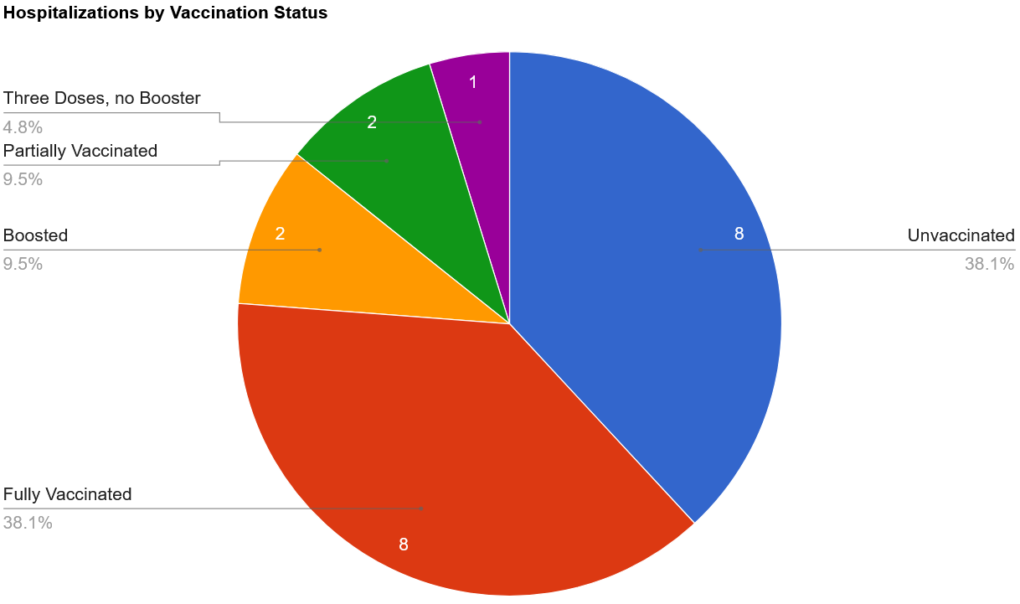
There were 27 total hospitalizations in the first two months of the year, with the majority of them (21) occurring in January. In order to hypothesize vaccine efficacy against hospitalization, we are forced to remove 5 of these cases where the vaccine status was left blank. We also should remove the 1 case where the vaccination status was listed as “Not in WAISS,” bringing us down to 21. (WAISS stands for Washington State Immunization Information System, and, according to Public Health, has only been consulted for a small number of cases. Vaccinations that were administered outside of the state or by the military are not recorded in WAISS.)
There were 8 cases in those listed as unvaccinated; 8 in those who were fully vaccinated; 2 in boosted individuals; 2 partially vaccinated, and 1 who had received three doses but was not boosted (likely immunocompromised). Totaling these up, we have 8 cases in the unvaccinated, 2 in the partially vaccinated, and 11 in those who had “completed their primary series.”
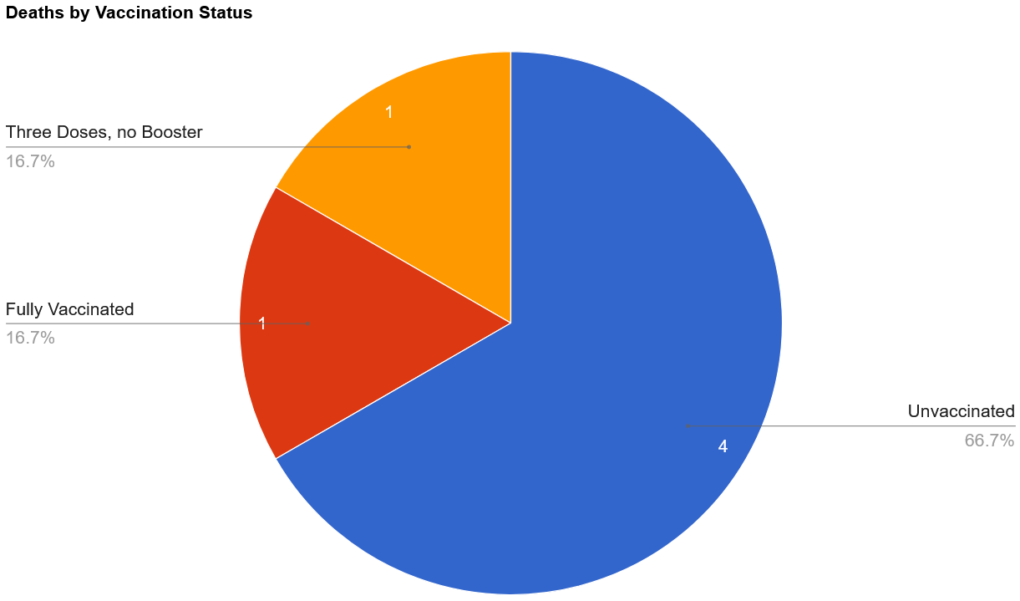
There were only 6 deaths, all of them the result of cases that were added to the official count in January. Of those, 2 of them lacked data on vaccination status, 2 were listed as unvaccinated, 1 of them had 3 doses but was not boosted, and 1 was fully vaccinated (no info on booster).
I was surprised to find missing data on vaccination status for hospitalizations and deaths. Hospitalizations and deaths are much more severe outcomes than just having a case of COVID. How could such important data be missing? In response to a query about this disparity, I was told that that vaccination status information likely simply “didn’t get updated on the line list when workloads were very high.” (This is also the reason why there are so many blank cells for cases.) However, even though this data is absent from the spreadsheet, it was reported on in The Leader. Parsing the information shared with The Leader by Public Health with the data in the spreadsheet, it becomes evident that the 2 instances where vaccination status was not listed occurred in unvaccinated individuals.
Interestingly (or perhaps as expected), there’s a theme undercutting all of these deaths. According to The Leader, the first death, a man in his 80s, was unvaccinated and had chronic health conditions.The second death, a woman also in her 80s, was unvaccinated and had chronic medical conditions.The man in his 70s (who had received three doses) was said to have active cancer. The remaining three individuals also all had “chronic medical conditions.” In other words, 100% of the people who died during the Omicron surge (January-February) had chronic medical conditions.
Nevertheless, the percentage of deaths in the unvaccinated (66.7%) is much greater than expected; the percentage of unvaccinated hospitalizations (38.1%) is also quite a bit higher than anticipated. This suggests that the vaccine may have an effect at preventing Omicron-related hospitalizations and deaths.
However, there are confounding factors at play here, as well. One of the most important problems to consider is that we don’t know that any of these individuals actually had the Omicron variant. It’s quite possible that some, or perhaps even all, of them were hospitalized or died with the Delta variant. Recall that all of the deaths occurred in January, closer to when the Delta variant was still the main variant in the community. This is important because the two variants are different in terms of mortality, and a vaccine that protects against one variant isn’t necessarily effective in warding off another.
Regardless of how effective the vaccines were against the Delta variant, there is a general consensus that they are very much less effective against Omicron; in fact, Albert Bourla, CEO of Pfizer, noted in an interview on January 10 that “two doses of a vaccine offer very limited protection, if any” against the Omicron variant. The company is also working on the development of a new vaccine, which wouldn’t be necessary if the current ones were effective against the Omicron variant.
We must also consider the small sample size of the groups. With only 20 hospitalizations (with known vaccination status) and 6 deaths, it is difficult to draw meaningful conclusions. One additional or fewer death could shift the percentages by a considerable amount.
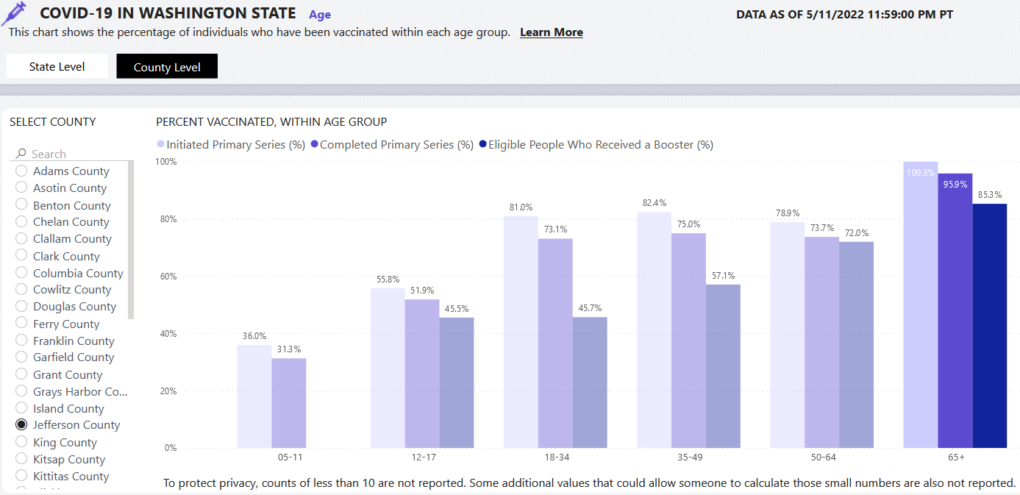
Perhaps even more importantly, we must consider the health of the two groups. Jefferson County is home to a large population of elderly, democratic voters, a group which has shown itself to be very likely to get vaccinated. In fact, if we look at the county-level data on the “Who is getting vaccinated?” tab of the DOH COVID-19 data dashboard, we can see that 100.3% (!) of those over 65 in Jefferson County have at least initiated vaccination. While this is, of course, impossible, and possibly an error resulting from an incorrect population estimate, it does suggest that very few of our county’s seniors are unvaccinated. Indeed, 85.3% of those who were eligible went on to get their booster dose.
Skepticism of the COVID-19 vaccines does not seem to be a thing among the elders of Jefferson County, and so one must ask the question, what might push someone not to get the vaccine? Does the very small number of unvaccinated hospitalization and deaths predominantly include people who had medical contraindications to getting vaccinated? Did a medical professional instruct these people not to get vaccinated because of their condition? When exposed to the virus, would people with chronic medical conditions be more likely to become infected (and thus have to be hospitalized and possibly die) than their healthier counterparts?
Our local Omicron data from January and February point in the direction of a vaccine that is slightly effective at limiting infection, and more effective at preventing hospitalizations and deaths. At the same time, however, there are large holes in the data set that, when filled in, could radically affect how the data could be interpreted. They also present a number of problems intrinsic to the method of data collection and a host of “what if?” questions that seriously hinder drawing any sound conclusions about the efficacy of these injectable products.
While raising more questions than answers, the local data hardly substantiates claims that the vaccines have been effective at preventing infection, hospitalization or death.
by Kincaid Gould | Oct 24, 2021 | General
When officials urge the public to “follow the science,” one would think that the appropriate data would be supplied. One would think that asking questions would be allowed. Regrettably, this is far from the case in Jefferson County.
Jefferson County Public Health (JCPH), the Leader and the Peninsula Daily News are the main print sources disseminating COVID-19 information for our county. While the data they publish can provide limited insight into the local COVID situation, there are many aspects of their reporting that are questionable, either because they don’t publish certain data or because they publish misleading data.
For example, data from the Leader indicate that more than half of Jefferson County “COVID deaths” have been in fully vaccinated individuals. That number may be as high as 71%. JCPH’s data also suggests cases among not fully vaccinated individuals outnumber those among fully vaccinated individuals three-to-one. However, this claim relies on misleading data. On the contrary, since early August, more than 40% of Jefferson County cases have been in fully vaccinated individuals. When data is muddled, irrelevant or misrepresented, it is impossible to make sound public health decisions— which, unfortunately, is exactly what Jefferson County Health Officer Allison Berry claims to be doing.
JCPH publishes a daily report with COVID-19 statistics for the county. Recently, I took a look at their data and was struck by the realization that some meaningful data can be extrapolated from some of the misleading statistics they’ve posted. That data, along with some other observations, is presented in the remainder of the article. All data is accurate as of 10/22/2021.
“Fully vaccinated” designation is misleading
The main source of my frustration within JCPH’s data is a pair of statistics (found in the third and fourth rows of the right-most data table): “Percent of cases among (not) fully vaccinated individuals since 2/1/2021.” At first glance, this might seem like an important and informative statistic. After all, this is the clearest data we have locally that informs on whether or not the vaccine actually prevents infection, right? As it turns out, this data is very misleading.
One important aspect to consider is the dichotomy between “fully vaccinated” and “not fully vaccinated”. What exactly do these terms mean? According to the CDC, one isn’t considered “fully vaccinated” until 14 days after they’ve received their last COVID-19 shot — either the single J&J, or the second of the two-dose mRNA jabs. Everybody else is considered “not fully vaccinated,” even if they’ve been “partially vaccinated.”
If all of the shots in a series (and the boosters) are the same, then one would think that being even partially vaccinated would confer some immunity. If being partially vaccinated provides any increase in immunity, there is absolutely no reason why those cases should be included in the same category as individuals who have received no shots.
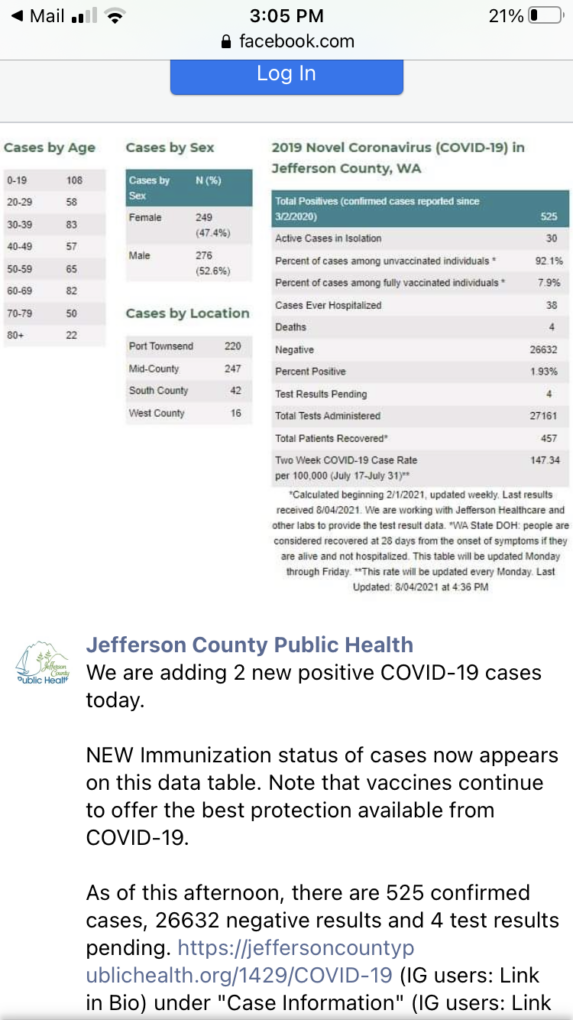
These two groups seem to be incorrectly interpreted as vaccinated vs unvaccinated by some people—in fact, JCPH was guilty of doing so on 08/04/2021 (see the screenshot). The Peninsula Daily News has run articles that reference these statistics and call the “not fully vaccinated” group “unvaccinated”. While there may be some unvaccinated individuals in the group, it is disingenuous to assume that all of them are. The data provided by JCPH leaves us guessing—it could be a 20-80 split among partially vaccinated and unvaccinated individuals for all we know!
Jefferson County Public Health 8/4/2021 Facebook post
Another problem is that these percentages are measured since 02/01/2021. At this early date, the vast majority of people were not vaccinated, nor were they eligible for vaccination. Most Washington state adults weren’t able to get vaccinated until April 15th, some two and a half months later. Furthermore, if somebody got vaccinated on April 15th and got all of their shots as soon as possible, they wouldn’t be considered “fully vaccinated” until late April (if they chose the J&J shot) or late May (if they received one of the two-dose vaccines).
Why does this matter? Measuring this data from a time when hardly anybody was or could be vaccinated against COVID-19 artificially inflates the number of cases among the “not fully vaccinated’ while decreasing the number among the fully vaccinated. Think about it this way — 0% of COVID-19 cases were found in vaccinated individuals in March 2020. Does this mean that the vaccines are effective? Of course not: the vaccines weren’t available then! Measuring since February 2021 is much better than March 2020, of course, but vaccines were still virtually inaccessible at the start of February.
Speaking of vaccine unavailability, children under the age of 12 are still ineligible for these experimental shots. If the statistics showing the percentage of cases among fully vaccinated and not fully vaccinated individuals is meant to show the vaccine’s efficacy at preventing infection, positive tests among those ineligible for vaccination shouldn’t be included. (I’ll come back to this point later.) Nevertheless, positive tests in this age group are still figured into the data. JCPH lists 151 positive tests among children aged 0-11 since they started collecting data in March 2020. That’s more than one tenth of local cases!
How could this data be improved?
For one, split the data into three categories: fully vaccinated, partially vaccinated, and unvaccinated.
Second, children aged 0-11 should be removed from this specific statistic, as positive tests within this population can’t possibly show the efficacy of the vaccines. This statistic should only include people who are eligible for vaccination at the time when they contract COVID-19. (Previous data should be adjusted to reflect this as well.)
Third, the start date of the data collection should be changed, measuring from May 1st at the very earliest. Better yet, JCPH could publish the percentage of cases among the three groups over a moving time frame. (For example, JCPH publishes a “two-week COVID-19 case rate per 100,000” containing data from the latest two-week period.)
JCPH first published the breakdown of the percentage of positive tests by vaccination status on 08/04/2021 and has updated the statistic at fairly regular intervals ever since. (This data can be found on JCPH’s Facebook page.) Because the percentages among fully vaccinated and not fully vaccinated populations are periodically updated (as is the total number of positive tests), the number of cases among these two populations since 08/04/2021 can be calculated by noting the change in percentages. This data provides a picture of the situation in Jefferson County during just the two-month period from August to October.
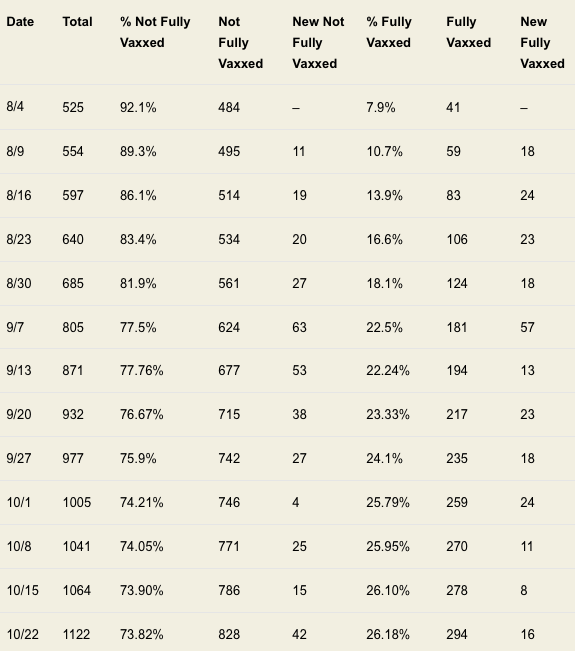
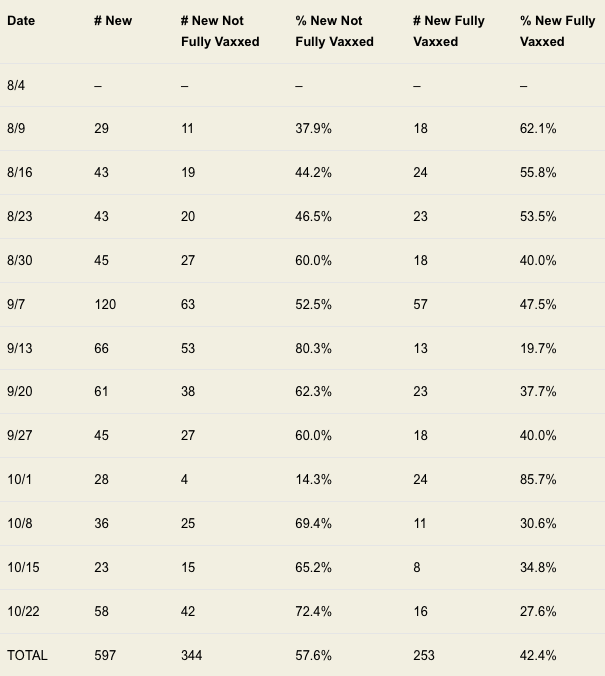
I have created two data tables from JCPH’s updates. The first displays the raw data reported by JCPH, and the total number of cases among the two populations during the period. The second table uses the same information, but removes any cases from before 08/04/2021. Additionally, it presents the percentage of cases added each week in the two groups.
TABLE 1 – Cases Among Not Fully Versus Fully Vaccinated
TABLE 2 – New Cases Among Not Fully Versus Fully Vaccinated
There is a clear trend in the percentage share of cases among the two groups since 02/01/2021. As Table 1 shows, the percentage of cases among the not fully vaccinated decreased from 92.1% to 73.82% over the time period, while the percentage among fully vaccinated individuals rose from 7.9% to 26.18%. One possible explanation for this trend is that the data is greatly skewed by the odd start date; this argument is further supported by the fact that even during weeks where there were more cases among not fully vaccinated individuals than among fully vaccinated individuals, the percentage of cases among fully vaccinated individuals increased (for example, during the week of 10/08/2021).
Table 2 makes the data much more clear. Over the period from 08/04/2021 until 10/22/2021, 42.4% of positive tests were among fully vaccinated individuals while 57.6% were from individuals who were either unvaccinated or partially vaccinated. These two percentages are worlds away from the 92.1% and 7.9% rates reported in August. They’re even considerably different from the percentages reported on 10/22/2021 (73.82% vs 26.18%). A 47.64 percentage point difference between 73.82% and 26.18% is more than three times greater than the 15.2 percentage point difference between 57.6% and 42.4%. The differences between these statistics evidently varies greatly with the time frame.
Let’s also consider improper inclusion of ineligible age groups.
On 08/18/2021, JCPH started reporting positive tests with an age band of 0-11-year-olds (replacing an earlier 0-19 age band). As of 8/18/2021, there were 62 individuals in the 0-11 category. By 10/22/2021, there were 151 cases in 0-11-year-olds. Subtracting 62 children from 151, at least 89 individuals aged 0-11 were diagnosed with COVID-19 in the larger period between 08/04/2021 and 10/22/2021. These cases shouldn’t be used to give an idea of vaccine efficacy, as the individuals couldn’t be vaccinated.
Subtracting 89 cases from the “not fully vaccinated” category for the data from 08/04/2021 until 10/22/2021, there are then only 508 total cases, among them 255 cases among the not fully vaccinated population and 253 among the fully vaccinated population. The percentages are virtually identical, with only two more cases found in not fully vaccinated individuals. (Remember that this is a conservative estimate, as there were very likely cases in 0-11-year-olds during the two-week window from 08/04/2021 to 08/18/2021.)
Saying that the vaccine prevents you from catching the virus is misinformation.
The vaccine companies only claim that the vaccine can reduce symptoms, hospitalizations and deaths. Unfortunately, JCPH doesn’t publish the data that could be used to support those claims. The number of asymptomatic and symptomatic cases is not shared (and possibly unknown). The number of fully vaccinated, partially vaccinated and unvaccinated hospitalizations is not reported. Information (e.g., comorbidities, vaccination status, age, date of death, etc.) surrounding alleged COVID-19 deaths is similarly unavailable.
Death data can be extrapolated from articles in the Leader, however, which show that 10 out of 17 ‘COVID’ deaths have been among the fully vaccinated. (Two deaths among the unvaccinated occurred in 2020 and should be discounted when considering vaccine efficacy; a third death reported in mid-April didn’t specify vaccination status. A more accurate number would thus be 10/15 deaths among the fully vaccinated (66.67%), or even 10/14 (71.43%)). It is unclear if the Leader uses the same definition of “unvaccinated” as the Peninsula Daily News (i.e., “not fully vaccinated”) or if it actually means unvaccinated. It is also unclear whether these individuals died of COVID-19 or simply with COVID-19.
If anything, I feel like the points raised above and the data provided by JCPH raise many more questions than they answer. If we are truly in the middle of a dangerous pandemic, shouldn’t the local health department be providing as much relevant and up-to-date information as possible? Are statistics showing the share of males and females who have contracted the virus (which have been divided at around 50-50 since March 2020) really more important than the percentage of deaths and hospitalizations that were among the unvaccinated, partially vaccinated and fully vaccinated?
Keeping information from the public prevents us from “following the science,” and sharing misleading information/pro-vaccine propaganda prevents us from seeing what’s really going on.