by Dr. Rob Rennebohm | Feb 10, 2023 | General
Editors Note: The following letter was sent by Dr. Rob Rennebohm to Public Health Officer Dr. Allison Berry and the Jefferson County Board of Health on February 4, 2023.
—————————————-
On November 16, 2022, I sent an email to Dr. Berry, Dr. Locke, and members of the Jefferson County Board of Health (BOH – Greg Brotherton, Kate Dean, Heidi Eisenhour, Amanda Grace, AJ Hawkings, Kees Kolff, Libby Wennstrom) to alert them to an important medical article entitled, Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19.
The article, written by German pathologist Dr. Michael Mörz, is a case report of autopsy findings in a 76-year-old man who had died three weeks after receiving his third vaccination against COVID-19. The article was published by the peer-reviewed journal Vaccines on October 1, 2022.
Dr. Mörz’s article provides compelling and sobering evidence of the potential of mRNA vaccines to cause serious harm to the brain and heart – namely, vasculitis, necrotizing encephalitis, and myocarditis. In my view, his report represents one of the most important to be published during the pandemic because of its potential to appropriately change attitudes about the mRNA vaccine safety.
I attached the Mörz article in my email to the above-mentioned physicians and BOH members. I also attached my own analysis of the Mörz article to help non-physicians to more easily understand its significance. I asked the BOH a series of pointed questions about possible vaccine-related immunopathology, the informed consent process, and the BOH’s continued promotion of the COVID vaccination campaign.
I was hoping that my email would stimulate and facilitate a healthy, scientific dialogue about the safety and wisdom of the COVID mass vaccination campaign — a dialogue that would inform and benefit all involved, including the general public. I requested a response from the BOH “within 2 weeks (i.e. by Nov 30), if possible.”
Local Health Authorities Ignore Physician’s Concerns About Brain and Heart Damage Linked to COVID Vaccines
Unfortunately, as described in my article published by the Port Townsend Free Press on December 9, 2022, I never received any response from any physician or staff or member of the BOH — not even a brief email saying, “Thank you for calling our attention to this article.”
Public Comment & BOH Meeting Response
Because of this lack of response, I decided to personally attend the Jefferson County BOH meeting on January 19, 2023. During a 15-minute segment set aside for “comments from the public,” I was given 3 minutes to again state my concerns about the significance of this article and to ask the physicians and BOH members for their thoughts about the article. I pointed out that no one had responded to my email of November 16, 2022.
Dr. Berry explained that the physicians and BOH members had “briefly talked about” the article among themselves. Dr. Berry emphasized that the article represented a single case report that, “notably,” had been published “in a ‘pay-for-play’ journal, which is the lowest quality of journals that we have.” She pointed out that the article’s findings “had not been replicated elsewhere in high quality research” or “in the valid peer-reviewed literature.” In her view, these observations about the article “called into question the accuracy of the findings.” For these reasons Dr. Berry and the BOH had decided not to take any further action regarding this article.
Unfortunately, the rules of the “public comment” segment of the meeting are that the citizen making the public comment is not given any opportunity to respond to the response of the members of the BOH. In other words, actual dialogue is not permitted.
After the brief public comment segment was over, the BOH members proceeded with their business meeting. After about 30 minutes of listening to that business meeting, I decided to leave. I had considered waiting until the end of the meeting to possibly engage Dr. Berry in further discussion of my concerns. But I decided it would be better to respond in writing, rather than be perceived as “confronting” the BOH.
My Written Response to Dr. Berry & BOH
Well-trained physicians use their critical thinking skills and medical knowledge base to develop their own opinion regarding the quality, value, and significance of a published article. If they humbly conclude that their knowledge base is too limited to perform an adequate assessment of the article, they seek help from more knowledgeable colleagues.
When I initially read the Mörz article, including the methods section and a careful look at the numerous images, it was immediately obvious to me that his analysis was scientifically sound and of very high quality. As a rheumatologist who has published extensively on the neuropathology of Susac syndrome, I could easily see for myself the lymphocytic infiltration (inflammation) surrounding vaccinal spike protein in the microvasculature and parenchyma of the heart and brain.
Well-trained physicians also double-check their conclusions, even when they feel quite certain, particularly when much is at stake. Accordingly, I double-checked my conclusions by sending the Mörz article to two of North America’s most knowledgeable and experienced neuropathologists. Both concluded that the article was excellent, scientifically sound, and that the author had drawn appropriate and important conclusions.
In comparison, how did the BOH and its physicians approach the article? Did they strive to develop their own independent opinion about the article? Then, if they felt their knowledge base was inadequate, did they seek the opinion of experts in the field? Did they bother to carefully read my written analysis of the article, which I painstakingly wrote to help non-pathologists interpret the article and its images?
Apparently not. Instead, they concluded the following (and I am paraphrasing):
It is a single case report so not much significance can or should be attached to it. It is not necessarily representative. In fact, even if the autopsy was excellently performed and the findings accurately interpreted, the pathologist may have simply stumbled upon an extremely rare event. There is no need to further address this article or Dr. Rennebohm’s concerns.
Yes, it is a single case report. But it is the one of the best-documented studies of its kind to look for the spike protein in an autopsy and try to determine whether it is derived from the vaccine or from natural infection. In 100% of autopsies that have been studied in this fashion, these abnormalities were found. That, of course, does not mean these findings are common, but it certainly means that this observation needs to be taken very seriously and absolutely warrants immediate further investigation — to promptly determine more exactly how common these findings are.
The responsible response to this article would be to double-check its excellence and significance by obtaining the opinion of objective experts in the field. If its excellence and importance are confirmed, the responsible response would be to thoughtfully and carefully share its findings with the public — out of an abundance of caution — which is our moral and medico-legal obligation as part of informed consent and human decency.
One could also argue that this single case report should at least prompt us to strongly consider stopping all COVID vaccination, at least of children and healthy young adults — until further similar autopsies are done. It is irresponsible to conclude that since this is a single case report, its findings need not concern us, need not influence our thinking about the safety of the vaccine, need not obligate us to change our message to the public, and need not modify the information we provide the public as part of our informed consent process.
Should “Open Access” Journals Be Discounted?
Regarding their conclusion that: It was published, “notably, in a ‘pay-for-play’ journal, which is the lowest quality of journals that we have.” Its findings “have not been replicated in the valid peer-reviewed literature.” These observations “call into question the accuracy of the findings.”
There is a great deal wrong with the above conclusion.
For one thing, the important question is “what is the quality of the article,” not “what is the quality of the journal in which the article is published.” The fact is, excellent articles may be found in journals that are considered “low quality” journals, and very poor articles can be found in “highly reputable” journals.
It is also important to point out that there is a considerable difference between journals that have a “low impact score” and journals that are of “low quality.” A journal that has a low impact score can, nevertheless, be an excellent journal or at least publish excellent individual articles.
Journals with “high impact scores” and reputations for “high quality” – like the New England Journal of Medicine, Lancet, and British Medical Journal – can and have published articles on COVID-19 that are of extremely low scientific quality and even fraudulent and retracted, whereas relatively obscure “low impact” journals have published articles on COVID-19 that have been excellent, scientifically sound, and extremely important (like the journal Vaccines in this case).
So, just because an article has been published in a relatively obscure medical journal that does not have a “high reputation” or a “high impact score,” does not automatically mean that the article is not of high scientific quality. Furthermore, during this COVID-19 era, it must be realized that “highly reputable” medical journals have been very hesitant to publish scientifically excellent articles, if those articles contradict the prevailing COVID narrative.
It is naïve to think that “highly reputable” medical journals have not refused to publish certain articles. If a physician or scientist submits an article that supports the prevailing narrative and its mass vaccination campaign, that article is much more likely to get published than an article of even greater scientific merit that provides sound scientific evidence that contradicts the prevailing narrative.
This is not a “conspiracy theory;” it is a reality that has been experienced by many physicians and scientists who have dared to challenge the prevailing narrative. Many scientists and physicians who have challenged the prevailing narrative have not only had their submitted manuscripts rejected, but have also been threatened with loss of employment, even loss of licensure. That is a fact.
So, one reason why an excellent scientific article might be published in an obscure journal with a low impact score, rather than in a highly reputable/high impact journal, is that the latter journals have been hesitant or unwilling to publish an article that raises questions about the merits of the prevailing narrative. In many cases, the author of an excellent article may need to publish it in an obscure journal by default. That is a fact.
It is also wrong, and insulting, to insinuate that an article has been published in an “open access” journal, because the article did not merit publication in a more reputable “closed access” journal, and/or because the author needed to pay a journal in order to get the article published. Such an assertion insinuates that the author is bribing the journal to publish an unworthy article and the journal is willing to accept such a bribe. Such an insinuation is insulting to both the author and the journal.
“Open Access” Journals Provide Open Access!
A major advantage for publishing in “open access” journals is that their articles will be free to anyone (including ordinary citizens) to read. Journals that are not “open access” force readers to either have a paid subscription to the journal or pay a fee to view the article. That fee is in the range of $30-50 per article. Since “open access” journals do not receive revenues from subscriptions or fee-for-read, they have to charge the author a publishing fee to cover the journal’s costs of publication.
Some authors purposefully choose to submit their article to an “open access” journal because they want the public to be able to read their article for free. Publication in an open access journal is a more democratic way to provide information and provides greater opportunity for ordinary citizens to read an important article. Publication in a “closed access” journal discriminates against and disadvantages those who cannot afford to shell out $30-50 to read a single article.
In fact, it is cruel to insist that people who are desperately seeking health information must pay in order to obtain it. The entire concept of “closed access” goes against the concepts of “health equity” and “health care is a human right,” not to mention the concept of common decency. It is misleading to portray “Open access” journals as “pay-to-play” journals. Again, it is insulting to insinuate that authors choose an “open access” journal “because it allows them to pay a journal to publish an unworthy article.”
The above discussion points out the importance of evaluating the scientific quality of the article itself, not the quality of the journal in which the article is published. If the article is scientifically excellent and important, it does not matter if it is published in an “open access” journal that is relatively obscure and has a “low impact” score — especially, if another reason for the excellent article appearing in an obscure journal is that “highly reputable” journals are not willing to publish articles that challenge the prevailing narrative.
BOH Needs to Focus on Safety Signals, Not Journal Prestige
Did the physicians and BOH members take the above complexities into consideration when they discussed the Mörz article? Did they focus on the scientific quality of the article itself (which is obviously excellent to anyone who knows what vasculitis looks like or bothers to ask more knowledgeable colleagues for help)? Or did they simplistically conclude that it is not a worthy article because it was published in an lesser known journal that requires authors to contribute to the coverage of publication costs?
The facts about the Mörz article are:
- This article is excellent. It is scientifically sound, and its findings are obvious and of profound significance and urgent importance.
- Even though it represents a single case report, the proper conclusion is that this single report is of such great concern that it should be carefully shared with the public, should result in immediate further study, and should raise the question of whether COVID-19 vaccination should be halted until more is known — at least in children and young, healthy adults.
- At the very least, the information provided in the Mörz article should become part of the informed consent process that physicians and health departments are legally and morally obligated to provide (but which is not being provided).
It is worrisome that the physicians and BOH members were not able to recognize the obvious scientific excellence and obvious significance/importance of the Mörz article. It raises questions about what else they may not be recognizing or understanding. Good, well-trained physicians are able to recognize obvious vasculitis, or ask for help if they are uncertain about the findings and quality of an article.
It is also worrisome that the physicians and BOH members were unable or unwilling to think of several possible explanations for the appearance of this article in the journal Vaccines, rather than in a “more prestigious” journal. Well-trained physicians consider more than one possible explanation when evaluating a problem. They don’t just think of one possibility (one diagnosis) and jump to that conclusion; they construct a differential diagnosis (carefully consider all plausible explanations).
It is worrisome that the physicians and BOH members concluded, simplistically, that they did not need to take any further action in response to this article: they did not need to share its findings with the public, or engage in dialogue with those who are concerned about the article’s findings, and/or change their thoughts about the mass vaccination campaign.
Good, well-trained physicians recognize “safety signals” that warrant immediate attention and further study, even if those signals might turn out to be rare, especially when the incidence of worrisome side effects is quite unclear. Good, well-trained physicians practice “anticipatory medicine” and take potentially worrisome signals seriously. Well-trained physicians thoroughly educate the public and provide true informed consent.
BOH Needs to Invite Dialogue, Not Discourage It
Let me emphasize that a fundamental principle of science and medicine is that challenges to the prevailing wisdom should be welcomed and respectful scientific dialogue should be strongly encouraged. My November 16, 2022, email represented an invitation for such dialogue. But no dialogue occurred. The BOH and its associated physicians did not even show the courtesy of responding in any way to my email. Their only response was silence.
When, two months later, I made a personal appearance to discuss the article, there was again no opportunity for dialogue. I was given three minutes to state my concerns. Dr. Berry and the BOH had as much time as they wanted to respond to my concerns; I was given no opportunity to respond to their response.
That, by definition, is not dialogue. They had all the power; I had none. That is not equity. That is not democracy. These represent gross violations of fundamental principles of science, use of power, and practice of democracy.
If a physician:
- is not able to recognize obvious vasculitis on their own, or does not bother to seek help to evaluate an article that they feel unable to adequately assess by themselves;
- is unable to recognize an excellent scientifically sound, profoundly important article;
- does not consider multiple plausible explanations for why a particular article is published in a “low-impact” journal;
- is not able to recognize worrisome “safety signals” and/or is unwilling to act on those signals;
- is unable to recognize medical information that must be shared with the public, or refuses to carefully share that information with the public;
- fails to fulfill their obligation to provide true informed consent;
- shows no interest in engaging in scientific dialogue;
- simply regurgitates the group think narrative handed to them by the authorities;
…then that physician has either not been well-trained (regardless of where they received their public health education) or is not practicing what they were taught. In either case, such a physician is failing miserably to serve the public.
Such a physician is a danger to the public and should not be in a position of power over the public’s health.
Has Mass Vaccination Prolonged the Pandemic?
Finally, let me add this: I was prepared for the possibility that the BOH’s response to the Mörz article would be: “Yes, the article raises legitimate concerns about the safety of the COVID vaccines, but we are convinced that the overall benefits of the vaccines, particularly at a population level, have far exceeded the risks.”
Those who make the above argument fail to understand that the mass vaccination campaign itself has prolonged the pandemic and made it far more dangerous. They fail to understand that in the final analysis, more lives will have been lost cumulatively (over the past 3 years and in the many months ahead) because of the COVID-19 mass vaccination campaign than if it had never been implemented in the first place — that is, if we had relied, instead, on the competency of the immune system.
The prevailing COVID narrative’s argument that “far more people would have died” if the COVID mass vaccination campaign had never been implemented, is scientifically and mathematically inaccurate. Far more people are going to end up dying because of the mass vaccination campaign, compared to the cumulative number that would have died if the campaign had never been implemented. The argument that “the benefits of the vaccine are so great that we must accept some ‘extremely rare’ side effects in some unfortunate individuals” is scientifically unsound.
Unfortunately, those who insist on promoting and obediently following the prevailing COVID narrative do not realize that this narrative and its mass vaccination campaign are based on a woefully simplistic understanding of the immunology, virology, vaccinology, evolutionary biology, and glycosylation biology involved in the COVID situation. The prevailing narrative and its mass vaccination campaign are scientifically unsound and unacceptably harmful — at both an individual and population level..
See the following companion articles for more information about the consequences of the misguided COVID mass vaccination campaign and why it continues to be far more harmful than helpful:
What is the Current State of the COVID Situation?
What is the Current State of the COVID Pandemic?—Part 2
Analysis of the Current COVID-19 Situation in China
Creating Social Beauty in Response to Abusive Silence
Responding to Abusive Silence by Creating Social Beauty
How Would Three of Canada’s Greatest Historical Figures Respond to the COVID Situation, If They were Alive today?
Pediatricians, Internationally, Please Call for an Immediate Halt to the Global Campaign to Vaccinate Children Against COVID
An Open Letter to Parents and Pediatricians—Part I
Open Letter to Parents and Pediatricians—Part II: A Review and Update
Open Letter to Parents Regarding COVID Vaccination—Part III: Questions to Ask Your Physician
Open Letter to Parents and Pediatricians—Part IV: The Harmful Immunologic Consequences of Vaccinating Children Against COVID
by Dr. Rob Rennebohm | Dec 9, 2022 | General
Dr. Michael Mörz, a pathologist in Germany, has recently published an article entitled, Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19. The article is a case report of autopsy findings in a 76-year-old man who had died 3 weeks after receiving his third vaccination against COVID-19.
This case report was published by the peer-reviewed journal Vaccines on October 1, 2022 (Vaccines 2022, 10, 1651).
Dr. Mörz’s article provides compelling and sobering evidence of the potential of mRNA vaccines to cause serious harm to the brain and heart — namely, vasculitis, necrotizing encephalitis, and myocarditis. His article may prove to be one of the most pivotal articles to be published in the conventional medical literature during the COVID-19 pandemic—because of its potential to change attitudes about the safety of mRNA vaccines against COVID-19.
To summarize the Mörz article, to present its pathology images in a way that might be more understandable to the general public, and to underscore the importance and implications of the article, I have written a Summary and Commentary about Dr. Mörz’s article.
Here is a link to the long version of the Summary/Commentary.
Here is a link to a shorter version of the Summary/Commentary.
The shorter version has been published on Dr. Geert Vanden Bossche’s website and republished on the Trial Site News website and on Dr. James Lyons-Weiler’s substack.
The shorter version of the Summary/Commentary is reprinted below.
—————————-
My email to Dr. Allison Berry, Dr. Tom Locke, and members of the Jefferson County Board of Health regarding the Mörz article:
On November 16, 2022, I sent the email below to Jefferson County’s Health Officer, Deputy Health Officer and members of the Board of Health (BOH), to alert them to the Mörz article and its significance. As you can see, I asked them to respond to several important questions. I requested that they respond within two weeks (by November 30).
It is now December 8, 2022. I have received no responses from Dr. Berry, Dr. Locke, or any members of the BOH. I have not heard a single word from any of them — not even a courteous, “Thank you for sharing this information. We will respond to it as soon as possible,” which would have taken less than 20 seconds to type.
The lack of response to this extremely important article is disappointing, to say the least. Perhaps, they are still engaged in the process of studying the article and carefully discussing it among themselves and, perhaps, with outside experts. But if that is the case, the professional and courteous thing to do would be to let me know that they are in the midst of that process.
Perhaps, the article is too complicated for them to understand, making it difficult for them to respond. But that is why I wrote the Summary/Commentary and wrote it in such a way that non-physicians could understand the article and its significance. Again, the professional and courteous thing to do would be to let me know that they are working on a response.
Perhaps, they think the article does not represent good science and simply represents misinformation/disinformation. But if that is the case, the professional and courteous thing to do is engage in scientific dialogue with me, during which they could explain their criticisms of the article and we could learn from each other.
Perhaps, they do not want to challenge their long-held COVID beliefs and understandings by considering new information. Perhaps it is too difficult, too uncomfortable (emotionally and psychologically) for them to consider a reversal in their thinking and recommendations. But such rigidity goes against fundamental principles of science and medicine.
Perhaps, they concluded that this vaccine-related complication (if it is, indeed, related to the vaccine) is probably “very rare” and, therefore, “it is best not to scare the public” by mentioning it—“lest it unnecessarily frighten people from becoming vaccinated.” Such a conclusion, however, is irresponsible in at least two ways. First, they do not know how rare or not rare this complication is, nor does anyone else, because this represents the only autopsy in which a definitive test for presence of vaccinal spike protein has been performed. Second, even if this complication proves to be extremely rare (which seems unlikely to me), health care workers have a moral and legal obligation to comply with a proper informed consent process, which includes mention of even extremely rare potential side effects. Frankly, I suspect that if more autopsies are done, and if they include testing for presence of vaccinal spike protein, it will become evident that versions of this complication are common—particularly if electron microscopy is performed on the tissues.
Perhaps, they simply do not care. Perhaps, there are other reasons for their silence.
Whatever the reasons are for their silence, it is sad and instructive that the individuals who are most responsible for caring about the health of Jefferson County citizens have remained silent about such a profoundly important article.
I am not sure what our next step should be. What would readers of the PTFP suggest?
—————————-
Dear Dr. Berry, Dr. Locke, and members of the BOH,
As a pediatrician/pediatric rheumatologist (formerly at Cleveland Clinic) and as a resident of Port Townsend during the first year of the pandemic, I have been deeply concerned about the wisdom and safety of the COVID mass vaccination campaign, both nationally and in Jefferson County—especially the campaign to vaccinate infants and toddlers with the mRNA vaccines.
Policies regarding the COVID pandemic should be based on a deep scientific understanding of the immunology, virology, vaccinology, evolutionary biology, and the glycosylation biology of the COVID situation. This includes a deep understanding of the immunopathology that is emerging among the COVID-vaccinated—particularly the neuro-immunopathology (which was my specialty at Cleveland Clinic).
I have attached an extremely important article, recently published (in the peer-reviewed journal Vaccines) by an excellent pathologist in Germany (Dr. Michael Mörz). It provides compelling and sobering evidence that spike protein produced by the mRNA vaccines can end up in the endothelial cell lining of capillaries in the brain and heart; that this is closely associated with CNS vasculitis, necrotizing encephalitis, and myocarditis; and that these vaccine-associated phenomena can be fatal.
I have attached the Mörz article for your review. I have also attached a Summary (for the General Public) and Commentary on the Mörz article that I have written to help non-physicians to more easily understand the Mörz article and its significance.
I have some questions for all of you:
- What is your reaction to the Mörz article?
- Do you think the COVID vaccine is responsible for the neuropathology and heart pathology documented by Dr. Mörz?
- How worried are you about the possibility of vaccine-related neuro-immunopathology occurring in some who receive the COVID mRNA vaccine?
- To what extent do you, as the COVID health experts in Jefferson County, feel obligated to call this article to the attention of the public in Jefferson County?
- Should discussion of this article be part of the informed consent process?
- Do you think the Mörz article should cause hesitancy about continuing the COVID vaccination campaign?
- Is the Jefferson County Board of Health encouraging COVID vaccination of infants and children?
I would appreciate hearing back from you within 2 weeks (i.e. by Nov 30), if possible.
Finally, would you be interested in organizing a Town Hall meeting in PT to discuss this article—so that the public could learn about the article and its significance? I would be happy to be a guest speaker at such a meeting.
With Warm Regards,
Rob Rennebohm, MD
—————————-
(Dr, Rennebohm’s article published on Dr. Geert Vanden Bossche’s website, Trial Site News website and Dr. James Lyons-Weiler’s substack.)
A Summary (for the General Public) and Commentary Regarding the Case Report Published by Dr. Michael Mörz:
Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19
By Rob Rennebohm, MD
November 10, 2022
Above is the title page of an article written by Dr. Michael Mörz, a pathologist in Dresden, Germany. Here is the link to the full article: (https://www.mdpi.com/2076-393X/10/10/1651). It is a case report of autopsy findings in a 76-year-old man who had died 3 weeks after receiving his third vaccination against COVID-19. This case report was published by the peer-reviewed journal Vaccines on October 1, 2022 (Vaccines 2022, 10, 1651).
Dr. Mörz’s article provides compelling and sobering evidence of the potential of mRNA vaccines to cause serious harm to the brain and heart—namely, vasculitis, necrotizing encephalitis, and myocarditis. His article may prove to be one of the most pivotal articles to be published in the formal conventional medical literature during the COVID-19 pandemic—because of its potential to change attitudes about the safety of mRNA vaccines against COVID-19.
To summarize the Mörz article, to present its pathology images in a way that might be more understandable to the general public, and to underscore the importance and implications of the article, I have written a Summary and Commentary about Dr. Mörz’s article.
Here is a link to the Summary/Commentary:
https://notesfromthesocialclinic.org/a-summary-for-the-general-public-and-commentary-regarding-the-publication-by-dr-michael-morz/
Take Home Visual images:
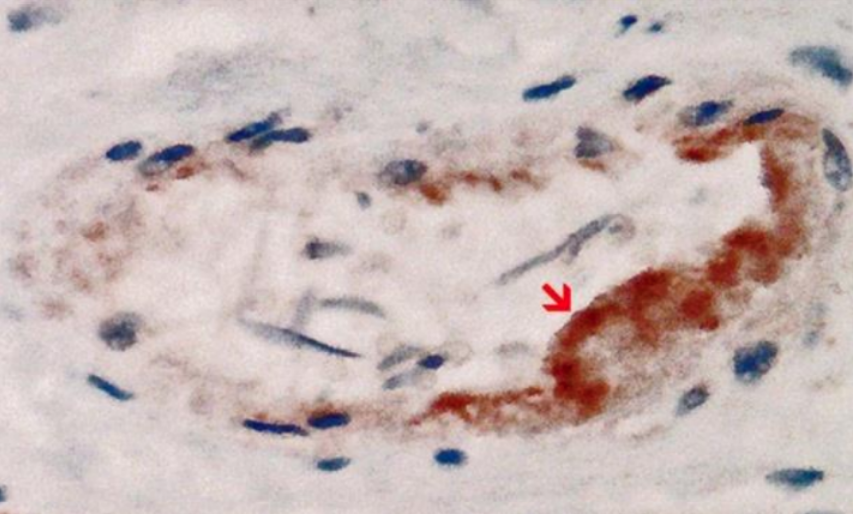
The above image (from the Mörz article) shows a cross section of a capillary in the heart. It demonstrates the presence of an abundant amount of spike protein (the brown material to which the red arrow points) within endothelial cells, which are the cells that line the inner wall of the capillary. There is endothelial cell swelling, and there are a few mononuclear inflammatory cells within the wall of the capillary. The spike protein was demonstrated to be of vaccinal origin, not from SARS-CoV-2 infection.
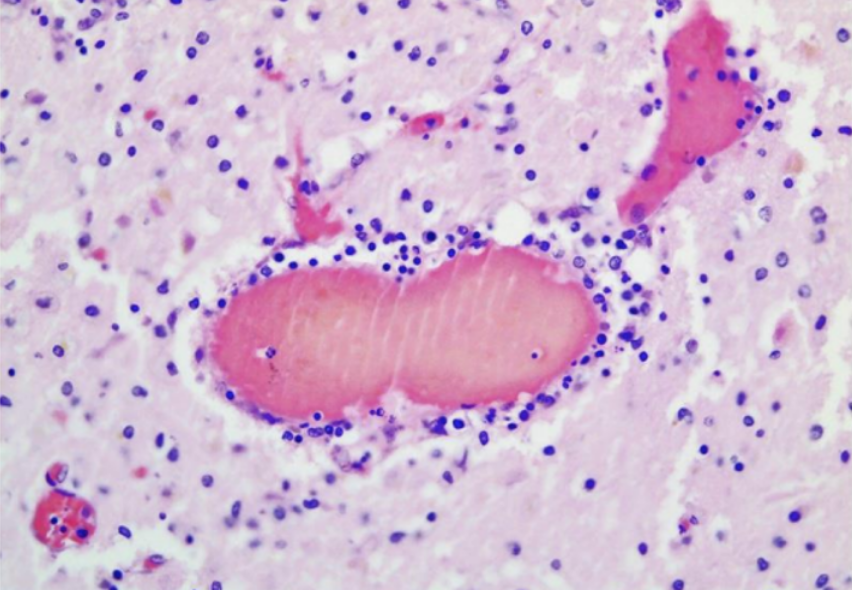
The above image (also from the Mörz article) is a cross section through a capillary in the brain. It shows prominent signs of vasculitis (inflammation of the blood vessel wall). The vessel is filled with hemolyzed blood, which is normal in autopsied cases. The many tiny blue cells that are present in the walls of the vessel (immediately surrounding the hemolyzed blood) include many lymphocytes (inflammatory cells). The presence of numerous lymphocytes in the wall of this vessel means that the vessel wall is inflamed—-i.e., the vessel is experiencing vasculitis.
The importance of the Mörz article:
Dr. Mörz has conclusively demonstrated the presence of an abundance of vaccinal spike protein in the endothelial lining of the walls of capillaries and arterioles in the brain and heart. He has also demonstrated significant inflammation within the walls of these same vessels. His interpretations of the findings are accurate and not overstated. He has appropriately suggested that these two findings are linked—that the inflammation in the vessel walls (vasculitis) was most likely triggered by the presence of vaccinal spike protein in those walls.
Dr. Mörz has also conclusively demonstrated diffuse and multifocal inflammation in the brain tissue (encephalitis) and in heart muscle (myocarditis). The encephalitis was necrotizing—i.e., associated with death (necrosis) of brain cells (neurons).
The two images shown above (along with the several other images presented in the Mörz article) support the following hypothesis: When the mRNA (that is embedded in the lipid nanoparticle of the Pfizer/BioNTech COVID-19 vaccine) is injected into the arm, the mRNA finds its way (via the blood stream) into distant cells—in this case endothelial cells that line the small blood vessels in the heart and brain. (The vaccine does not simply stay in the arm.) Once in the endothelial cell(s), the mRNA instructs the ribosomes in the cell to manufacture spike protein. The spike protein then migrates to the outer surface of the endothelial cell. The immune system then sees the spike protein (or fragments thereof) on the surface of the cell, recognizes it as foreign, and concludes that the endothelial cell has become infected. Accordingly, the immune system sends lymphocytes and other inflammatory cells into the walls of the vessel to attack the presumed infected endothelial cell(s). The vessel wall becomes inflamed (vasculitis) and, during this process, the endothelial cells become immunologically injured and may swell to varying degrees. Sometimes, abnormal intravascular coagulation (clotting within the vessel) may be triggered. In some instances spike protein finds its way through the blood vessel wall and penetrates into the brain (or heart) tissue, where the spike protein may trigger an inflammatory reaction in the brain (encephalitis) or heart (myocarditis).
People who have been vaccinated against COVID-19 (and those contemplating vaccination) deserve to know whether the Mörz report of probable vaccine-induced microvascular and parenchymal (tissue) injury in the brain and heart represent extremely rare phenomena or are more common than that. Vaccinees and the public at large deserve to know the prevalence of such phenomena, and they deserve to know the full spectrum of such findings. If such phenomena are more than rare, our hope would be that the abnormalities are usually only minimal, not as dramatic as in the case reported. We would also hope that the abnormalities might be reversible, possibly amenable to treatment—particularly if patients are warned to not receive any further COVID-19 mRNA vaccination.
Scientific understanding of potential serious side effects of the mRNA vaccines—including knowledge of the prevalence, spectrum, and pathogenesis of such complications, and potential treatment options for them—would improve if more autopsies were performed in situations like that of the case reported by Mörz.
Physicians, nurses, hospitals, medical centers, health departments, the CDC, NIH, FDA, WHO, the American Academy of Pediatrics (AAP), the pharmaceutical industry, government leaders, and media outlets that have assured the Public that the COVID-19 vaccines are “very safe” owe it to the Public to thoroughly, openly, honestly, publicly, and prominently discuss Dr. Mörz’s article and its implications. To date, there has been no mention of this article by the CDC, NIH, FDA, WHO, AAP, Pfizer, Moderna, government leaders, the mainstream media, or the medical experts who routinely inform the Public. On the contrary, instead of halting the mass vaccination campaign (which is the scientifically and morally correct thing to do), the promoters of the COVID mass vaccination campaign are currently re-doubling their efforts to greatly increase vaccination rates—spending billions of dollars to maximize vaccination against COVID-19, even among infants and toddlers.
To those people who have been encouraged, pressured, even mandated to receive COVID vaccination—physicians and scientists owe a massive top priority collaborative effort to thoroughly study the pathogenesis (the causative chain of events that lead to disease) and potential treatment of vaccine-induced endotheliopathy, vasculitis, encephalitis, and myocarditis—even if these complications prove to be rare. The death of the 76-year-old man reported by Dr. Mörz should not go in vain. We need to determine how to promptly recognize and promptly provide optimal early treatment for vaccinated people who may be developing early evidence of similar complications in their brain, heart, both, and/or elsewhere.
In the meantime we should deeply thank Dr. Mörz for performing and publishing his extensive and careful study of this one patient. The scientific quality of his work is excellent. His careful article represents a major contribution to medicine and Humanity. He is to be commended for the expertise, time, effort, and courage it took to present this compelling and valuable information. He has superbly honored the best traditions of science, medicine, and ethics and has performed a great service to Humanity. We should also commend the journal Vaccines for demonstrating the wisdom and moral courage to publish Dr. Mörz’s article. Like Dr. Mörz, Vaccines has honored the best traditions of science, medicine, and ethics, and has honored Humanity in the process.
Rob Rennebohm, MD
Pediatrician and Pediatric Rheumatologist
Retired (formerly at Cleveland Clinic)
Email: rmrennebohm@gmail.com
Website: www.notesfromthesocialclinic.org
by Dr. Rob Rennebohm | Feb 7, 2021 | General
As a pediatrician and pediatric rheumatologist who has published peer-reviewed articles on COVID-19, I would like to comment on the importance of knowing the Ct value at which a SARS-CoV-2 PCR test becomes positive. [The Jefferson County Health Department is not releasing this information. See our earlier article at this link. The Editor]
The PCR test for the SARS-CoV-2 virus is a good test when it is properly manufactured, properly conducted, used in an appropriate setting (e.g., in the evaluation of inpatients with COVID-like clinical features), and properly interpreted by carefully and fully taking Ct values into account.
It is not a reliable test when used in the screening of asymptomatic (or only mildly and non-specifically symptomatic) individuals, if the test is positive only after 33 or more cycles of amplification and this full information is not reported to patients and their physicians.
Ct = Cycle threshold; Ct = the number of amplification cycles needed before the test detects presence of viral material in a specimen. The higher the number of amplification cycles needed before detection of viral material occurs (i.e., the higher the Ct number), the lower the viral load and the less sick and contagious the person is likely to be.
If a test becomes positive after only 12 amplification cycles (i.e., positive at a Ct of 12), the viral load is very high—approximately 100,000,000 copies per microliter. [1-3] If the test becomes positive after 22 cycles (at a Ct of 22), the viral load is approximately 2,500,000 copies/mL. [4-5] If the test becomes positive only after 37, 40, or 45 amplification cycles, the result most likely represents either a false positive, or a true positive due to only a trace amount (less than 100 copies, even just 1-3 copies) of inert, non-contagious, “dead” SARS-CoV-2 viral debris (assuming the test is truly capable of always accurately identifying such a tiny amount of viral debris). [2, 6, 7]. Rarely, a positive test at a high Ct is identifying an asymptomatic person who has very recently become infected and might soon have a high viral load (low Ct), but this possibility can be evaluated by carefully following the person and repeating the test within 3-4 days, to see if symptoms develop and/or the Ct drops.
Unfortunately, it is very difficult to know with certainty whether a positive result at a Ct of 33 or higher represents a false positive or an accurately identified trace amount of SARS-CoV-2 viral material. The test was not designed to be reliably accurate after so many amplification cycles. When the test is used in an appropriate setting and the test is positive at a Ct of 30 or less, the false positivity rate is probably less than 4% (perhaps only 1-2%, as the test manufacturers claim). However, when the test is used in a surveillance setting and is “positive” at a Ct of 33 or higher (particularly at 37 or higher) the exact false positivity rate is currently unknown and likely to be quite high—probably as high as 70%. [6, 7]
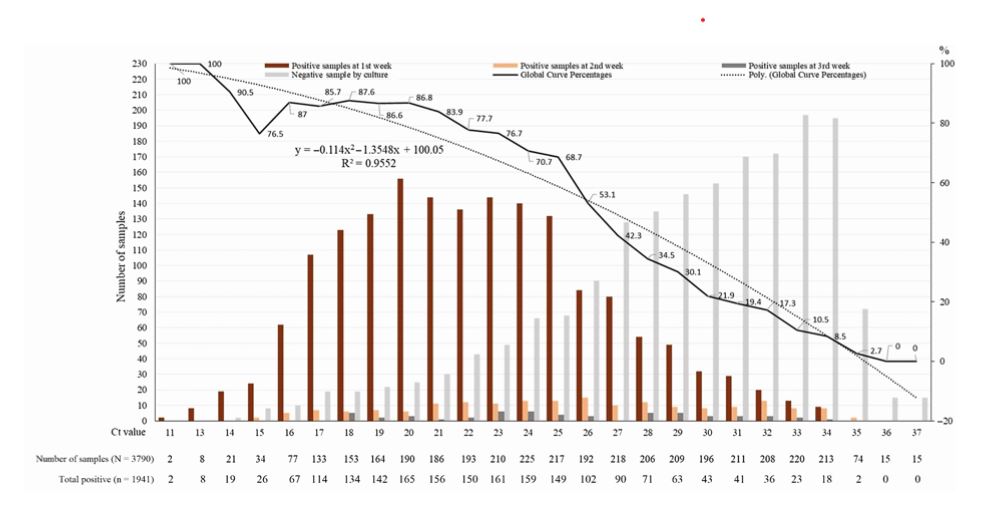
Based on what is currently scientifically known, it is best (most accurate) to label any test result that is “positive” at a Ct higher than 32 as an “inadequately interpretable” result. It is not scientifically sound and, in fact, is misleading and harmful, to label people with a positive test at a Ct of 33 or higher as a “new COVID-19 case.” More accurately, they are people with an “inadequately interpretable” result who, furthermore, are unlikely to be infectious [2, 8]. Regarding this latter point, please see Graph 1 (after the References section), which points out that it is extremely unlikely that a person with a positive test at a Ct >35 is infectious.
For the above reasons, experienced PCR scientists recommend stopping the PCR test after 30 (or 32 at the most) amplification cycles, because positive results obtained after 32 or more cycles are unreliable (inadequately interpretable) [2] and are not associated with contagiousness [2, 8].
Unfortunately, to date, SARS-CoV-2 PCR tests have been reported only as being positive or negative, with no indication of how strongly or weakly positive. Although Ct results have always been available for each individual test (since the beginning of the pandemic), Ct results have not been routinely reported or used for clinical or epidemiological purposes. This has been the case throughout the USA and most of the world.
It has also been unfortunate that most SARS-CoV-2 PCR tests are set to perform 40, 45, even 50 amplification cycles in their effort to detect viral material. (This varies from one test kit to another—see Table 1 after References.) That is, if a person’s specimen is negative after 30 amplification cycles, further cycles are, nevertheless, performed (up to 50 cycles with some tests), looking for evidence of tiny amounts of viral material. Only if no viral material is detected after 40, 45, or 50 cycles (whichever number the test system sets as the stop point) is the test declared negative. Even if a test becomes positive only after 45 or 50 amplification cycles, it is declared a positive test (without any mention of the Ct value) and the person tested is declared a “new COVID case.”
The Jefferson Healthcare Lab uses the XpertXpress SARS-CoV-2 PCR test, which is set to perform 45 amplification cycles before stopping its effort to detect SARS-CoV-2 viral material.
When a person is told they have a positive SARS-CoV-2 PCR test, they deserve to know how strongly positive their test is and what their result means. Does their result mean they are carrying a huge viral load, are very contagious, and should be very worried about themselves and those with whom they have been in contact? Or are they carrying only a tiny amount of dead, non-contagious viral debris that represents no threat to them or others? Or are they in a pre-symptomatic phase, with a low viral load that could soon accelerate? Or does their result represent a false positive?
The Ct value at which a person’s test is positive can shed considerable light on the above critically important questions. But, again, to date, Ct values of positive tests have not been made available to patients, physicians, public servants, or the public.
Having emphasized the importance of knowing the Ct value at which a test is positive, it is important to also emphasize that there are limitations to the information provided by the Ct value. The Ct value is not a true quantitative test of viral load; it just provides a rough and indirect (but, nevertheless, very helpful) estimate (a good, educated guess) of what the viral load might be. It is true, too, that if the same specimen is tested with 3 different COVID PCR tests each might be positive at a different Ct value (e.g., at a Ct of 16 in one test, 20 in another test, and 22 in the third—but not at 37 or 45 in one of the three). For these reasons Ct values need to be interpreted with caution and in clinical context, particularly until more data on Ct values of positive tests have been collected and fully analyzed.
In the meantime, it is far better to have a COVID PCR test report that includes the Ct value at which the test was positive, than to have a report that only says positive (or negative) without any Ct information provided. Though imperfect, the estimate of viral load offered by the Ct value is far more valuable than no estimate at all, especially if the Ct value is carefully interpreted and placed into clinical context.
When in early November the CDC reported that 100,000 “new COVID cases” (meaning new instances of a person having a “positive” SARS-CoV-2 PCR result) were occurring per day in the USA, neither the individuals with the positive tests, their physicians, their public health departments, the CDC, the NIH, WHO, Johns Hopkins University, or the public knew what percentage of those 100,000 tests were positive at a Ct >32 and what percentage were positive at a Ct of 30 or lower—because, to date, the Ct values at which tests have been positive have not been reported or taken into consideration.
It would be enormously beneficial if we, as a nation, were to report, study, clinically use, learn from, and base public dialogue and public policy (at least in part) on the Ct values of positive tests. This would include retrospective and prospective reporting of the Ct values of all positive tests. We could at least start doing this in Jefferson and Clallam counties and, thereby, lead the nation in doing so. We would be doing the nation a great service.
Medically, morally, and ethically— individuals with positive PCR tests, as well as physicians, epidemiologists, public policy makers, and the public— deserve to know, and need to know, the Ct value at which a SARS-CoV-2 PCR test is positive. Without Ct information, interpretation of the number of “new COVID cases,” “new COVID hospitalizations” and “new COVID deaths” is severely compromised, as is public policy and the care of individual patients.
From now on, when a person is told that their SARS-CoV-2 PCR test is positive, they and their physicians would be wise to ask, “At what Ct value was the test positive?” And when the public is told that 100,000 new COVID cases have been occurring per day, the public and their public servants would be wise to ask, “What percentage of those 100,000 were positive at a Ct of 33 or higher (particularly a Ct of 37 or higher)?”
Such questions and their honest answers would facilitate healthy public dialogue and stimulate much-needed critical thinking—both of which are essential for successful resolution of the COVID-19 pandemic. True science and true democracy depend on such critical thinking and healthy, informed, public dialogue.
For further, more detailed discussion of Ct values, including caveats about Ct information, please see my original article, “The Importance of Knowing the Ct Value at which COVID PCR Tests are Positive,” which may be found on the “Notes from the Social Clinic” website: https://notesfromthesocialclinic.org/the-importance-of-knowing-the-ct-value-at-which-covid-pcr-tests-are-positive/
REFERENCES:
- Tom MR, Mina MJ. To Interpret the SARS-CoV-2 Test, Consider the Cycle Threshold Value. Clin Infect Dis. 2020 May 21: ciaa619. Published online 2020 May 21. doi: 10.1093/cid/ciaa619
- TWiV 640: Test often, fast turnaround, with Michael Mina. https://youtu.be/kDj4Zyq3yOA
- Your Coronavirus Test is Positive. Maybe it shouldn’t be. Interview with Michael Mina, MD. Published August 29, 2020; Updated September 17, 2020. https://www.nytimes.com/2020/08/29/health/coronavirus-testing.html
- Bryan A, Fink SL, Gattuso MA, et al., SARS-CoV-2 viral load on admission is associated with 30-day mortality. Open Forum Infect Dis. 2020 Dec; 7(12): ofaa535. Published online 2020 Nov 3. doi: 10.1093/ofid/ofaa535
- Perchetti GA, Nalla AK, Huang ML, et al. Validation of SARS-CoV-2 detection across multiple specimen types. J Clin Virol. 2020; 128:104438. doi: 10.1016/j.jcv.2020.104438
- Francesca F, et al. Detection of SARS-COV N2 Gene: Very low amounts of viral RNA or false positive? J Clin Virol. 2020 Dec; 133: 104660. Published online 2020 Oct 14. doi: 10.1016/j.jcv.2020.104660.
- Katz AP, et al. False positive reverse transcriptase polymerase chain reaction screening for SARS-CoV-2 in the setting of urgent head and neck surgery and otolaryngologic emergencies during the pandemic: Clinical implications, Head Neck 42 (7) (2020) 1621–1628, https://doi.org/10.1002/hed.26317
- Jaafar R, Aherfi S, Wurtz N, et al. Correlation Between 3790 Quantitative Polymerase Chain Reaction–Positives Samples and Positive Cell Cultures, Including 1941 Severe Acute Respiratory
Syndrome Coronavirus 2 Isolates, Clinical Infectious Diseases, ciaa1491, https://doi.org/10.1093/cid/ciaa1491
GRAPH 1: Percentage of positive viral culture of SARS-CoV-2 PCR positive naso-pharyngeal samples from COVID-19 patients. No sample that was positive at a Ct >35 had a positive culture. (Reference 18: Jaafar R, Aherfi S, Wurtz N, et al. Correlation Between 3790 Quantitative Polymerase Chain Reaction–Positives Samples and Positive Cell Cultures, Including 1941 Severe Acute Respiratory).
TABLE 1:
The number of amplification cycles that various commercial SARS-CoV-2 PCR Tests are set to perform in their effort to detect viral material:
- Gnomegen: 39 cycles
- GK: 40 cycles
- In Bios-Aires: 45 cycles
- Xpert Xpress: 45 cycles
- Luminex: 45 cycles
- Quest: 50 cycles