by Ana Wolpin | Mar 31, 2021 | General
In late February, I received an email from a Port Townsend friend about her 85-year-old aunt’s rapid decline following her first shot of Pfizer’s experimental mRNA vaccine.
“My mom and I have been taking care of my aunt. When she got the shot [on February 15], she had just graduated from physical therapy because she was so strong and able to get up from being seated without using her hands for help, walk with a cane for an hour slowly, feed herself no problem, talk about memories. Since the 15th she has been dramatically declining, especially in the last five days… to where she now cannot walk at all, she can’t really control movement of her torso, cannot feed herself, cannot discern reality from hallucinations, and is incontinent and can get very angry. We had to make the difficult decision to have emts come yesterday morning to take her to the hospital (she had slithered to the floor and we could not get her up) and we insisted they admit her because we cannot care for her safely in this condition.”
A week later, her aunt was dead. What my friend witnessed mirrors reports of devastating injury and death around the world from these injections, particularly among the fragile elderly.
The photo above shows carloads of people lined up outside Jefferson Healthcare to receive experimental vaccines. The picture is different outside Jefferson County. Half of America–including healthcare professionals–is refusing the jabs.
Is my friend’s aunt the first Jefferson County fatality from this global experiment? Or has our county already seen, in a matter of weeks, more death by injection—which you are not hearing about—than the virus itself caused here in more than a year?
Stories like my friend’s are being ignored, downplayed, or denied by the mainstream media. But for anyone who looks beyond the incessant propaganda from the pharma-controlled narrative that the new Covid-19 vaccines are “safe and effective,” a far different story has emerged about this unprecedented medical experiment.
The prevailing narrative tells us that injuries following the jab are exceedingly rare and deaths are coincidental. But thousands of doctors, scientists and other experts have been sounding the alarm about this reckless experiment, often at great personal risk. Despite heavy censorship, vicious attacks, shaming and shunning, truth is increasingly coming to light.
This article will examine the counter-narrative urgently calling for a halt to all mass experimental injections.
Ignored and denied by mainstream media, global death and injury abound.
Just a sampling of reports you will not see on mainstream news:
Experimental vaccine death rate for Israel’s elderly 40 times higher than COVID-19 deaths
“While in January a group of independent doctors concluded that experimental COVID-19 vaccines are ‘not safer‘ than the virus itself, a new analysis of vaccine-related death rates in Israel demonstrates that this may indeed be the case to dramatic levels.” An analysis of data from the Israeli Health Ministry determined that “the mRNA experimental vaccine from Pfizer killed ‘about 40 times more (elderly) people than the disease itself would have killed during a recent five-week vaccination period’, and 260 times more of the young than what the COVID-19 virus would have claimed in the given time frame.”
Whistleblower: 25% of Residents in German Nursing Home Died After Pfizer Vaccine [click on link for video]
Disturbed by a facility-wide vaccination drive with military soldiers present, and the distressing patient deaths that followed, a Berlin nursing home caregiver came forward to provide testimony to attorneys from the German Corona Investigative Committee. The whistleblower describes how rather than peacefully slipping away as was normally seen with elderly patients he cared for, after their first dose of the Pfizer mRNA vaccine, seven of 31 residents with dementia died “as if they were tortured.” An eighth resident was near death at the time of the interview and died a few days later.
The long-time caregiver, sharing footage taken by a co-worker, says that reactions following the shot—“changes in behavior, strong fatigue, weakness, sudden gasping for breath with heart racing”—and the manner of the residents’ deaths were unlike anything he and his colleagues had ever witnessed before.
“Typically death was always peaceful for old people… their breathing was relaxed and their eyes stayed closed. This is very different death. It’s as if they cannot let go… their eyes are open, they are agitated, this strong tremor is changing their breathing. The pallor of their face is quite different. They are highly unsettled with this violent gasping for breath… a constant shaking of the upper body, this creepy, fearful gaze… it’s more of a struggle and it is not dying with dignity.”
When a second shot was forced on the 23 surviving residents just weeks after their first injection, another died and 11 more were seriously injured. (39 minutes, subtitled)
53 Dead in Gibraltar in 10 Days After Experimental Pfizer mRNA COVID Injections Started
Prior to the rollout of the injections, it is reported that over the preceding year only 17 people in total had died from Covid-19 in the small British Colony of Gibraltar (population 32,000). Within 10 days of starting Pfizer mRNA COVID injections, 53 were dead. “Tiny Gibraltar is like a petri dish; in no other place has there been such a brutally clear relationship between vaccine roll-out and increased ‘Covid deaths’.” Local media blamed the deaths on the virus, not the vaccine.
46 Nursing Home Residents in Spain Die Within 1 Month of Getting Pfizer COVID Vaccine
In Andalusia, Spain, 46 of 140 nursing home residents died in the wake of a Pfizer vaccination campaign. As in Gibraltar, their deaths were blamed on a “coincidental” outbreak of the virus, not the shots. In another nursing home in the same province, 22 elderly residents died following injections.
Similar alleged Covid outbreaks and death clusters following vaccination in Norway, Germany, England, Sweden. Scotland, Canada, and the U.S. are described here.
Vaccine injuries and deaths in the United States have followed the same pattern being observed around the world.
Closer to home
Knowing he was risking his career, Certified Nursing Assistant (CNA) James Develon could not remain silent after watching 14 of the nursing home residents he cared for die within two weeks after receiving the Pfizer experimental mRNA injections:
“They are dropping like flies.” [Click on link for video.]
CNA Develon reports that in 2020 there were “zero deaths” from Covid the entire year at the U.S. nursing home where he works. Following the shots, not only was there a rash of fatalities, but many other residents were near death. He describes the same spiraling loss of function my friend saw her aunt experience:
“People who were once walking are no longer walking. People who were once talking can no longer talk. People who were once able to think, can no longer think properly… delirium, confused.”
The deaths were explained away as resulting from the Covid virus—not the shots—from an unidentified “superspreader”. But that story didn’t add up, Develon said. Residents who had refused the injections were not sick; only the vaccinated were injured and dying. (5 minute clip at above link; full 47-minute video here).
32 Residents die from outbreak at Auburn nursing home.
As described in Robert F. Kennedy, Jr,’s article, Death by Coincidence?, “An Auburn, New York nursing home reported, without any apparent irony, that 32 of 193 residents have died since the facility began administering the Pfizer vaccine on Dec. 21. The company claims that its clients are dying of COVID-19 infections, not the vaccine.”
“Coincidence is turning out to be quite lethal to COVID vaccine recipients,” says Kennedy.
That is true not only among the high-risk elderly following vaccination, but in cases of healthy younger people dying directly after their shots as well.
- Sara Stickles, a 28-year-old healthcare worker from Wisconsin, broke out in rashes immediately after her second Pfizer shot. Five days later, severe headaches led to loss of consciousness, hospitalization, and an initial diagnosis of a ruptured brain aneurysm. A week after her injection she died when all brain activity ceased. [source]
- A 28-year old nurse’s aide in Iowa received a Pfizer vaccine at 11 am. He initially called in to work with a report of headache and dizziness, but decided to come to work anyway. He “was found down in a patient bathroom during his shift in our facility while taking care of a patient,” wrote a co-worker. He was coded, dying that day. [source]
- Most recently, an 18-year-old Illinois teen with no pre-existing conditions experienced headaches, body ache and fatigue the day after receiving a Moderna Covid injection. Two hours after complaining of chest pain on day three, he was found unresponsive and pronounced dead. [source]
Miscarriages are also being reported following these injections. Among scores of reports are:
- a 37-year-old woman in Washington state who lost her baby at 26 weeks the day after receiving her first Moderna shot; [source]
- a 32-year-old New Mexican woman, 22 weeks pregnant, who began having abdominal pain and vaginal bleeding after a second Pfizer shot and miscarried the next day; [source]
- a healthy Wisconsin woman, 29, just four weeks pregnant, who miscarried the same day she had her first Pfizer shot. [source]
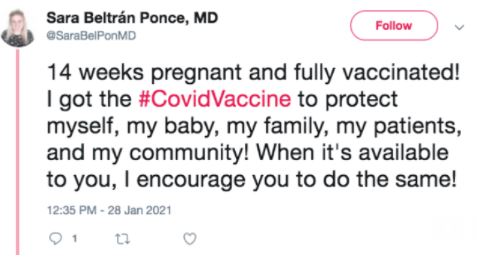
None of these nameless statistics made the news. However, the miscarriage of Wisconsin doctor Sara Beltrán Ponce, did. Dr. Ponce’s high-profile tweets exclaiming that at 14 weeks pregnant she was fully vaccinated—and urging everyone else to do their part, get the shot, protect the community—caused a stir on social media: “I got the #CovidVaccine to protect myself, my baby, my family, my patients, and my community! When it’s available to you, I encourage you to do the same!”
Just days later Dr. Ponce tweeted: “it’s with a heavy heart that I tell my #MedTwitter family that I’ve suffered a miscarriage at 14 1/2 weeks. My husband and I are devastated… Rest in Peace, angel… This is truly a sadness I didn’t know was possible to feel.”
Fauci: over 90% vaccine efficacy is “just extraordinary”!
Pharma’s Warp Speed trials prior to being granted Emergency Use Authorization (EUA)—not approval or licensure—were conducted on generally healthy people and were not transparent. The immune-compromised, those with co-morbidities, pregnant women, and children were excluded from the trials. Older adults and minorities, some of the hardest-hit populations, were significantly underrepresented, leaving many questions unanswered.
Investigators like British Medical Journal (BMJ) senior editor Peter Doshi are still asking for the raw trial data and challenging initial claims of efficacy based on the selective data hyped by the media.
“All attention has focused on the dramatic efficacy results: Pfizer reported 170 PCR confirmed covid-19 cases, split 8 to 162 between vaccine and placebo groups. But these numbers were dwarfed by a category of disease called “suspected covid-19”—those with symptomatic covid-19 that were not PCR confirmed. According to FDA’s report on Pfizer’s vaccine, there were ‘3410 total cases of suspected, but unconfirmed covid-19 in the overall study population, 1594 occurred in the vaccine group vs. 1816 in the placebo group’.”
Of the 43,448 low-risk trial participants who received injections, Pfizer used the minuscule subset of 170 symptomatic vacinees who were PCR confirmed to generate a media frenzy of headlines trumpeting an “extraordinary” 95% efficacy rate. Other vaccine developers followed their lead. Based on the far larger symptomatic Covid group that was revealed in the FDA report, Doshi calculates that there was an actual “relative risk reduction of 19%—far below the 50% effectiveness threshold for authorization set by regulators.”
He notes, “With 20 times more suspected covid-19 than confirmed covid-19, and trials not designed to assess whether the vaccines can interrupt viral transmission, an analysis of severe disease irrespective of etiologic agent—namely, rates of hospitalizations, ICU cases, and deaths amongst trial participants—seems warranted, and is the only way to assess the vaccines’ real ability to take the edge off the pandemic.”
Pharma’s trials, which were not designed to prove that the vaccines prevent infection, interrupt transmission, or reduce serious outcomes, appear to be an exercise in industry spin. The years of surveillance standard for licensing a vaccine have barely begun. An average approval process for any vaccine or biologic is normally between 7 and 10 years. The global campaigns underway, injecting nanotechnology never before deployed on human populations, are the true trials.
So how is post-vaccination damage from this giant experiment being monitored in the US?
Simple answer: it is not.
VAERS: Vaccine Adverse Events Reporting System
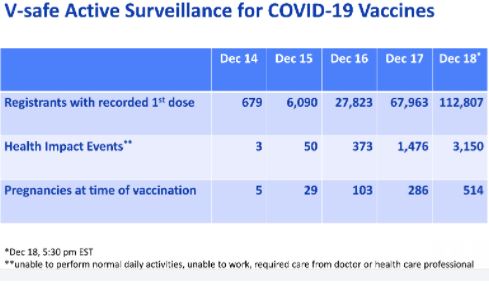
In the first days of America’s Covid vaccine rollout, December 14-18, 2020, the CDC conducted “V-safe Active Surveillance for COVID-19 Vaccines.” According to the CDC’s website, V-safe is “a smartphone-based tool that uses text messaging and web surveys to… tell CDC about any side effects after getting the COVID-19 vaccine.”
Over those five days, more than 5,000 “Health Impact Events” immediately following injections were identified. On December 18 alone, 2.79% of people who received first dose shots—3,150 out of 112,807—used this smartphone app to report reactions so severe that they were “unable to perform normal daily activities, unable to work, [and/or] required care from a doctor or other health professional.”
More than 60 million Americans do not own smartphones, and roughly half of senior citizens don’t use them. V-safe also excludes 25 million people in the U.S. with limited English proficiency; the app is only in English. Once again, two of the groups inadequately represented in pharma’s trials but being marketed to most aggressively—senior citizens and minorities—are also the most likely to not be able to use this reporting system.
So how many adverse reactions were NOT captured by this app-only surveillance?
Given the CDC’s reliance on a smartphone app for reporting vaccine side effects and injuries, the actual number of severe reactions might have been significantly higher. But the data gap gets even wider.
Despite being assured that this experiment would be closely monitored, our primary source of data since Dec. 18 has not come from V-safe Active Surveillance, but from VAERS—the CDC’s Vaccine Adverse Events Reporting System.
VAERS is a voluntary passive system, with no regulatory oversight, no requirement or incentive to report vaccine adverse events. The system is so flawed that in 2010, a Harvard study commissioned by Health and Human Services (HHS) determined that less than 1% of vaccine injuries and deaths are captured. Only a small percentage of the public, including those working in health care, even know it exists. And because adverse events are regularly attributed to coincidence or denied outright, even when medical personnel do know about the system, vaccine reactions regularly go unreported. Not only is there no incentive for health professionals to report to VAERS, it is notoriously difficult to use.
With the new, experimental Covid injections, there are further disincentives to attribute death or injury to vaccination and to file reports with VAERS. Families may not be able to collect on life insurance policies if a loved one dies by injection, or use their health insurance if injured. Not only is there complete liability protection from damages for vaccine manufacturers, health departments, hospitals and retail establishments, personnel who administer the shots, and policy makers, but many private insurers exclude coverage of these vaccines as well. Medical insurers have clauses such as “side effects arising from the COVID-19 vaccine are not covered under our exclusion for… experimental treatment.”
Among doctors, nurses, and other healthcare workers, there is tremendous pressure to deny any damage from the shot. As described by Bernadette Pajer of Informed Choice Washington, “A lot of the medical community are afraid that if it [an adverse reaction] happened to them, to speak out and report—because they have to be part of the system that pushes the vaccines.” And when Missouri Rep. Blaine Luetkemeyer questioned CDC Director Robert Redfield during a House Oversight and Reform subcommittee hearing on coronavirus containment, Redfield confirmed there were financial incentives to classify deaths as resulting from the virus, not other causes. Was there a “perverse incentive” monetary gain for hospitals to classify deaths as being coronavirus-related when the virus was not the actual cause of death?, asked Luetkemeyer. Redfield responded, “I think you’re correct in that.”
In my friend’s case, “This hospital [Jefferson Healthcare] has no way set up to document concerns and is not too interested from what I can tell.” She made the effort to report her aunt’s vaccine death to VAERS, but says the system was so difficult to navigate, “I couldn’t figure it out.”
She also asked her aunt’s attending doctor to report to VAERS and he said he would. If he did, she has received no follow-up. And it clearly was not reported as a Covid vaccine death—there is no mention of the vaccine as a causative factor on the death certificate or of the shot even being administered prior to her death. Her aunt’s cause of death is listed as “renal failure.” Our hospital and health department have not acknowledged it as a vaccine death, and the CDC has no record of it.… another vaccine casualty attributed to other causes, not captured by the system that we are relying on to assess safety of this new technology.
My friend’s experience is so common that organizations like Children’s Health Defense are offering additional resources to help people document vaccine injuries and deaths.
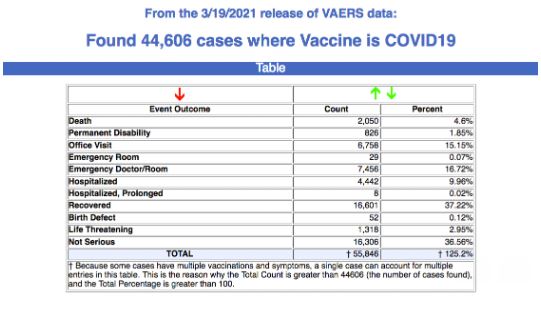
Even with the many disincentives and obstacles, as of March 19, VAERS data shows 44,606 reports of adverse events following Covid vaccines, including 7,095 serious injuries, and 2,050 deaths.
With 118.3 million vaccines administered, that is a 0.037% adverse event rate. Given that the initial V-safe Active Surveillance showed a “serious adverse reaction” rate nearly 100 times that—almost 3% (and that missed people who didn’t have the smartphone app)—the 1% capture rate found by the Harvard study would appear to be accurate. That would mean that in the past three months there may have been more than 4 million (4,460,600) actual adverse events, 709,500 serious injuries, and 205,000 deaths from Covid injections.
Like the death of my friend’s aunt, the vast majority of fatalities induced by the shot go unreported. They are instead attributed to infections from the Covid virus, or to heart attacks, strokes, or organ failure “coincidentally” following injections.
Likely causes for so much injury and death from this experimental injection will be explored in Part Two…. [which you can now read by clicking here]
by Ana Wolpin | Feb 20, 2021 | General
“Locke…is concerned about a Jefferson County group that may be spreading misinformation concerning the accuracy of the tests, claiming incorrectly that up to 90 percent of COVID-19 tests provide false positives.” [Peninsula Daily News, 2/7/21]
“Public naysaying on the spread of COVID-19 continued at Monday’s meeting of the board of county commissioners, with the public comment period being marked by more claims of false positive COVID-19 tests by some Jefferson County residents… ‘That kind of denialism is becoming more dangerous,’ Locke said.” [The Port Townsend & Jefferson County Leader, 2/3/21]
Who are these citizens being called dangerous by Jefferson County’s Health Officer, Dr. Thomas Locke? They are concerned citizens being censored by all media on the peninsula except the Port Townsend Free Press.
I am among them.
Dangerous Misinformation?
Over the past year, a group of local researchers has diligently examined data and analyzed information driving the global policies now devastating our world. Independent of our efforts, Stephen Schumacher was also deeply researching, coming to similar conclusions that much of the fear narrative being broadcast didn’t hold up to scrutiny.
In July 2020, Schumacher submitted a letter to the Port Townsend Leader citing statistics related to COVID-19 (Covid) lockdowns. His letter was withheld from publication for nearly a month, but eventually ran.
The following month, the Leader flatly refused to print his next letter. Unable to participate in the community opinion forum which “welcome[s] letters from our readers,” Schumacher then paid $500 to purchase ad space to share his information. A second ad, at the end of August, costing $550, warned about problems with the now-infamous discredited models Dr. Locke was citing to justify lockdowns. This was followed by two more ads regarding lockdowns in September and October.
In November, the Leader took censorship to the next level. After first accepting a paid ad about concerns over PCR tests, the publisher emailed Schumacher to inform him that they would not be running it. His ad featured a graph from a Harvard epidemiologist, and cited the Journal of the American Medical Association, the CDC, and other mainstream sources. In an email exchange asking why he was being censored, the publisher wrote, “We need to make decisions based on the best interest of our business.”
Was the payment Schumacher offered to exercise his right for freedom of expression insufficient when weighed against the newspaper’s role as a propaganda arm of Dr. Locke?
Schumacher took his rejected ad to the Peninsula Daily News. The PDN first agreed to accept his $530, then balked. The ad ultimately ran on Nov. 22. Several weeks later he attempted to buy ad space there a second time, but was told the publisher had rejected it. “When I asked if there was something specific I could have tweaked to make the ad acceptable, the answer was negative,” he said. “The content was verboten.”
PCR tests come into focus
While local censorship was ramping up, many scientists were expressing concerns that the PCR tests, responsible for exploding “case” counts and continued lockdowns, were not reliable. In some experts’ words, they are “not fit for purpose.” Most of this information was also being suppressed.
But on August 29, 2020, the New York Times published the story, “Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be.” It quoted Harvard epidemiologist Dr. Michael Mina: “from 85 to 90 percent of people who tested positive in July with a cycle threshold [Ct] of 40 would have been deemed negative if the threshold were 30 cycles.”
Evidence mounted that cycle thresholds are critical, confirming the New York Times story.
In a September article in Clinical Infectious Diseases, a French team looked at more than 100 studies on PCR tests. All studies found that above 30 cycles “patients could not be contagious as the virus is not detected in culture above this value.” They then performed 3790 of their own tests, reporting similar findings—of the samples that tested positive after 35 PCR cycles, 97% were negative upon viral culture. And of samples testing positive after 37 or more cycles, 100% were culture negative.
The lack of PCR reliability was reinforced in November by an international group of experts who formally challenged these tests as a valid diagnostic tool for identifying Covid cases. In their extensive report—“External peer review of the RTPCR test to detect SARS-CoV-2 reveals 10 major scientific flaws at the molecular and methodological level: consequences for false positive results”—the authors contend that serious defects in the test have “led to worldwide misdiagnosis of infections.” They conclude that the test is “completely unreliable” and “unsuitable as a specific diagnostic tool to identify the SARS-CoV-2 virus.”
In December, an Italian team documented that when the Covid PCR test is positive only at a high Ct value, the incidence of false positivity is at least 70%. Their article in the Journal of Clinical Virology warns that the detection of viral RNA at a high cycle threshold “needs to be interpreted with caution.”
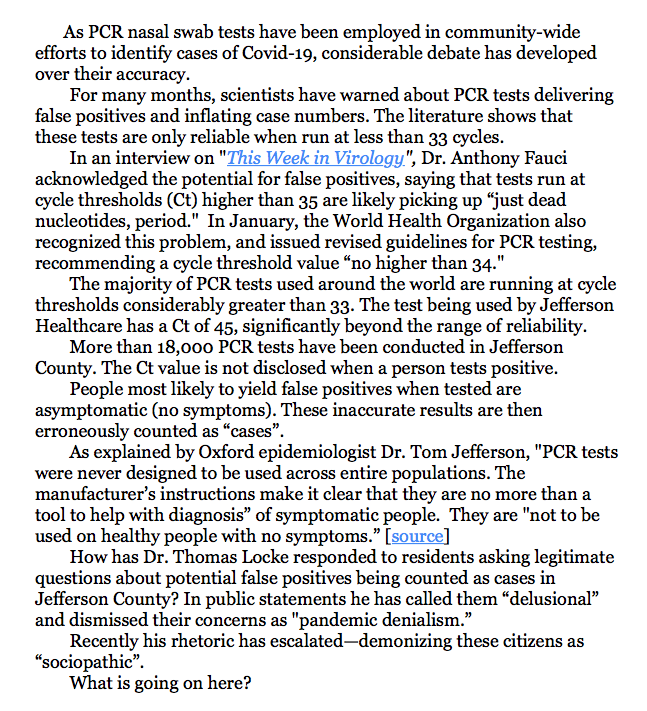
Revised guidelines from the World Health Organization followed in January. All parties agree that beyond 30-35 cycles, the PCR test cannot reliably provide accurate identification of a Covid case, calling into question case figures worldwide.
Is this incontestable global consensus—that at high cycle thresholds PCR tests yield mostly false positives—the “misinformation” that Locke speaks of in the PDN quote above?
As revealed by Annette Huenke in her Port Townsend Free Press article, “Is Jefferson County Health Department Overstating COVID Case Numbers?,” the cycle threshold of the PCR test being used in Jefferson County is not 30 or 35 or even 40. It is 45. No scientist disputes that with a positive result at 45 Ct, the chance of infection is zero.
Our test results do not report the cycle count; they merely declare a binary positive or negative. Without the Ct information there is no way to judge viral load, or if the test simply picked up dead viral debris; if the person is contagious, or if the result is a false positive.
Locke has yet to disprove any of this information.
Censorship and Demonization: the New Normal
For several months I have been among the citizens writing to our county commissioners about this concern. In response, the commissioners repeatedly defer to their expert, Locke. He waves off any responsibility, passing the buck to state authorities—not my problem—while insulting the citizens bringing these issues to light.
Locke’s attacks have grown increasingly shrill and aggressive towards residents challenging his pronouncements. In a response to a brief request from Annette Huenke asking for data he had referenced in a weekly report broadcast on KPTZ, Locke concluded his email with:
“And no amount of data will convince people who are consumed by pandemic denialism and wish to rationalize their pseudoscientific, sociopathic beliefs.”
In addition to the “pandemic denialism” pejorative he has been using for months, the county’s Public Health Director is now calling citizens who ask relevant, important questions “sociopaths”. It is no wonder that increasing divisiveness is pervading our community.
Our voice is censored by all local media except this online publication. When some of us raised the issue with our county commissioners of free speech being denied by the mainstream press, Commissioner Greg Brotherton rationalized that it was important to have “a unified approach” in messaging the public. That is a euphemism for “official propaganda only.”
The newspapers not only refuse to investigate valid citizen concerns, they allow no right of rebuttal to Locke’s messaging and name-calling.
On February 10, I submitted this letter to the Leader:
To date, the Leader has not run my letter.
12/23/20 protest outside office of PT Leader
Nor has a letter about PCR tests from Dr. Robert Rennebohm been published, submitted a week prior to mine. An MD who has extensively researched Covid issues, Rennebohm stresses the importance of disclosing Ct values in reporting new Covid cases, underscoring the need for and responsibility of public health departments to change course:
“Medically, morally, and ethically—individuals with positive PCR tests, as well as physicians, epidemiologists, public policy makers, and the public—deserve to know, and need to know, the Ct value at which a SARS-CoV-2 PCR test is positive. Without Ct information, interpretation of the number of “new COVID cases,” “new COVID hospitalizations” and “new COVID deaths” is severely compromised, as is public policy and the care of individual patients.”
Rennebohm’s detailed explanation of Ct values can be read in the Port Townsend Free Press article, The Importance Of Knowing The Ct Value At Which SARS-CoV-2 PCR Tests Are Positive.
But not even a credentialed physician, one who I daresay has greater understanding of PCR’s uses and limitations than Locke, is permitted to offer a professional perspective in the Leader if it diverges from Jefferson County’s Public Health Director. Rather than requesting interviews or promoting healthy debate on an issue that is profoundly impacting every one of us, there is only the silencing of any viewpoint that does not support the official narrative. A “unified approach.”
Valid, scientifically confirmed concerns should generate robust public discussion in our community. Instead, county residents are deluged with one-sided information that is often inaccurate and falls significantly short of adequately educating the public. Area newspapers, the local radio station, and other media provide a bully pulpit for Locke to disseminate what many scientists around the world would argue is misinformation.
Reporting all sides of a story is the fundamental purpose of journalism, the recognition that a fully informed citizenry is the foundation of democracy. That has been suspended in our New Normal. Allowing diverse voices to engage in civil discourse is deemed dangerous.
Cycle threshold values are only a small part of the PCR story, the one that has gotten the most attention. Equally critical is the clear instruction—in accordance with the PCR test’s authorized labeling—that its use should be limited to symptomatic individuals… not inflicted across entire communities of people who, for the most part, are not sick.
On January 4, the Food and Drug Administration released “Risk of False Results with the Curative SARS-Cov-2 Test for COVID-19: FDA Safety Communication.” The FDA’s direction to healthcare providers, patients and caregivers is that PCR test use should be “limited to individuals within 14 days of COVID-19 symptoms onset.” Use on asymptomatic people or outside the two-week window was likely to produce false results, or at least inadequately interpretable results.
The story in Jefferson County
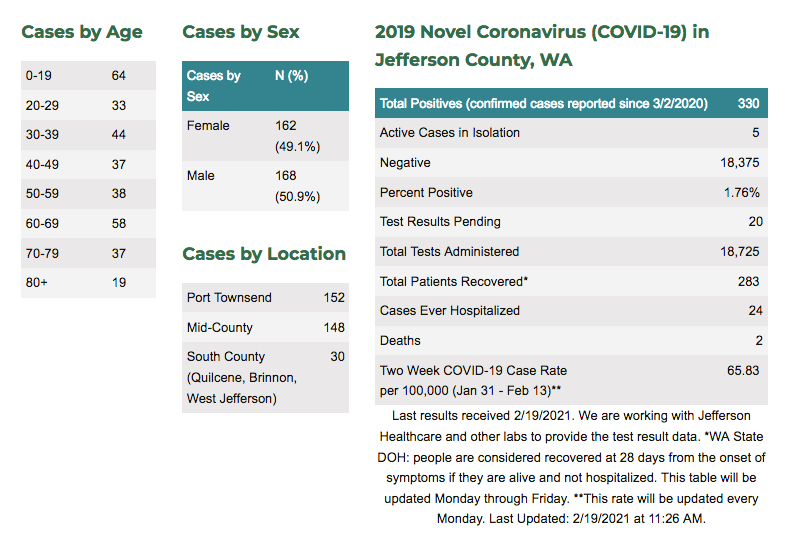
Of more than 18,700 tests administered in Jefferson County since March 3, 2020, over 300 cases have been identified as “positive” to date.
This includes symptomatic people—those with Covid symptoms like fever, body aches, and sore throat—who may have been tested within the 14-days-of-onset window.
It also includes people tested who had NO Covid symptoms—those who are in facilities or jobs that require testing; who go to the hospital for unrelated elective procedures; who are admitted to the ER after a heart attack, stroke, or accident; and those who ask to be tested out of fear, or curiosity—some of them getting multiple tests. None of these meet the criteria of showing symptoms in a 14-day window. Most of those tests are inadvisable and prone to false positives.
The only people with positive tests who can arguably be called legitimate cases are the first group—those who presented with Covid symptoms. As Dr. Tom Jefferson, the FDA and others have warned, PCR tests were not designed to be used randomly across general populations.
And these tests are not always reliable even in diagnosing symptomatic people. Without knowing the cycle threshold values of tests conducted, we have no clear data to identify true cases.
Over nearly a year, only two dozen of our Covid “cases” have been hospitalized. And even the people in that category likely included false positives. If a person was admitted to the ER due to a heart attack or stroke but tested positive for Covid, they were added to the county “case” tally and put in the Covid ward.
What is the real picture of Covid in our community? Of the 330 “cases” who received only a yes/no result from a PCR test that ran up to 45 cycles, how many test results were false positives? If the majority of people tested here were asymptomatic, how many of those with positive results were actually contagious?
Based on testing data the New York Times obtained from three states, only a tenth of the people counted as cases were true Covid positives; 90% were unnecessarily forced to isolate and submit to contact tracing. Jefferson County’s percentage of false positives may not be quite as high as those in Massachusetts, New York and Nevada. But without reviewing the Ct values of our test results, we simply do not know.
Why accurate case counts matter
In practical terms, being erroneously identified as a Covid case can have serious consequences. A false positive could result in your healthy teenager being quarantined for no reason, leading to suicidal ideation. Suicide rates have risen dramatically, especially among youth, since lockdowns were imposed.
Your own false positive might mean lost wages or damage to your business. Perhaps most harmful, though, is being stigmatized as a threat to other people’s safety. I know of people who felt perfectly healthy, but tested positive—likely false positives—and even after two weeks of quarantine, were treated like lepers by friends and co-workers afraid to be around them.
In a Daily Mail article, Dr. Tom Jefferson of the internationally acclaimed Cochrane Collaboration gives many examples of how people’s lives are being ruined by a similar testing regime in the UK:
“Last week I received an email from someone whose results have flip-flopped from positive to negative four times over two months, and another from a man who has been unable to see his elderly mother, isolated in a care home, because she continues to test positive week after week.” People, he says, “are at their wits’ end because they are testing positive for Covid-19 despite having recovered from their symptoms. Some never had symptoms in the first place but are still being told they have the virus long after any possible infection. They are anxious and confused. Their lives are on hold.”
At the extreme, being wrongly labeled a Covid case can kill you.
Say you are the person described earlier with no Covid symptoms and you have broken a bone. You are rushed to the ER and required to have a PCR test. A false positive result at a 45 cycle threshold places you in the Covid ward next to a contagious true-Covid-positive patient. Whereas your only actual medical issue is from your broken bone, you are now at risk of contracting Covid. And of dying— like the 80-year-old woman being counted as a Jefferson County Covid death. She was put in a Seattle hospital for complications due to surgery and is reported to have died from catching the virus there.
What has all this cost?
How much time, energy and resources have been spent for this massive testing program and the relentless propaganda campaign of ever-rising case numbers used to keep the public in fear?
What has been the true cost in Jefferson County? Much more than the money expended on 18,000+ tests and all the personnel involved. The impact on our community’s mental health, economic stability and social fabric is incalculable.
Dr. Tom Jefferson calls this deeply flawed testing program a “hugely expensive blunder”:
“I’d have to conclude that the official coronavirus figures have been grossly overstated, with all the damage that entails. Where appropriate we should carry out tests, but only in the context of symptoms, the date they first emerged, a history of recent contacts and any pre-existing medical conditions. I believe that Britain’s new-found testing mania is a retreat from properly conducted clinical medicine as well as from common sense. And that we are witnessing a triumph of herd thinking – an expensive one at that.”
Citizens have been terrorized week after week with alarming headlines about new case numbers, urging them to get their tests. Officials who have promoted this fear are deeply invested in the false story they have spun and the resources that have been wasted. No one wants to hear that they are responsible for such a massive error.
So the response is to shoot the messenger. Voices revealing the truth are censored, insulted, and vilified. In Jefferson County that is a coordinated effort between local media, the board of health, and our public health director.
We are now being told that censorship—the prohibition of free and open dialog—is justified. It’s for the greater good. These people are dangerous. And the more indefensible the narrative becomes, the more the censorship and attacks intensify.
PCR tests are being misused “to justify excessive measures such as the violation of a large number of constitutional rights,” writes Belgian physician, author and public health analyst Dr. Pascal Sacré. The assumption that a “positive RT-PCR test means being sick with Covid” is misleading, he says. Falsely equating positive tests with Covid cases is “the starting postulate, the premise of all official propaganda, which justifies all restrictive government measures: isolation, confinement, quarantine, mandatory masks, color codes by country and travel bans, tracking, social distances in companies, stores and even more importantly, in schools.” [source]
Are our leaders going to permit this misguided testing program to continue to fuel fear and inflict untold harm in our county? It is long past due for our local officials to put an end to this costly mistake.