by Annette Huenke | Jul 14, 2022 | General
This article is the first in a series that will shine light on the inner workings at our local hospital system. Administrators at Jefferson Healthcare would have us believe that all is well within their institution, particularly as they return to the taxpayers, hat in hand, to fund their next dream of upgrades to the Sheridan Street facility. With the backdrop of a looming global financial crisis, materials shortages and supply chain ruptures, how viable is this $100 million-plus gamble? What will it actually cost when all is said and done?
Jefferson Healthcare is struggling mightily to retain and recruit nurses and other patient-facing staff, and as this exposé will reveal, significant roots of that problem are internal. Through personal accounts from insiders, public records requests and investigation of current federal funding mechanisms, we will take a deep dive into the contemporary condition of Jefferson County’s hospital system.
——————————
“We concluded years ago that we are in the trust business… Hospitals are nothing but fancy buildings with expensive technology if we don’t have a great employee base. So we are very focused on — one, recruiting and bringing in the right people for our team, and then once they are here, working really hard to provide a work environment that is satisfying both personally and professionally and allow for providers to grow and develop.”
Jefferson Healthcare CEO, Mike Glenn at the May 12, 2022 Community Presentation
——————————
We have come to expect glowing reports of good deeds and great intentions when public agencies are selling a property tax increase. But how much truth is contained within Mike Glenn’s flowery assessment above? Is the view from the ivory tower the same as it is on the patient floors? What degree of “trust” exists within “the team” in the medical institution so many in this community count on?
Anyone who has lived here for long has personally, or has family and friends who have received stellar care at Jefferson Healthcare facilities. I have, my partner has. The nursing and support staff get rave reviews again and again, as do most providers.
However, the Free Press has been contacted on multiple occasions by hospital workers who feel an urgency to sound the alarm on what they see as chronic mismanagement that puts nursing staff and patients alike in potentially dangerous situations. The aim of this article is to give voice to those who have not been heard, despite their years-long efforts to improve the work environment through dialogue and negotiation. Management responds with platitudes like “let’s continue to work on solutions together…” as they neglect the reforms most requested by staff — regular schedules and part-time employment.
I sat down with one of those whistleblowers recently, and listened to her story. She’s asked that I use a pseudonym to protect her identity, understandably concerned about retaliation.
Suzanne is a Registered Nurse (RN) who came to work at Jefferson General Hospital over twenty years ago. She loves her work — that is to say, she loves taking care of people.
The era of healthcare facility mergers and acquisitions ushered in new and improved bean counters and fancy new nomenclature to distinguish upper management from the rest of the pack. Jefferson Healthcare birthed its own Strategic Leadership Group (SLG) approximately fifteen years ago. The current SLG is pictured below.
Strategic Leadership Group (from top left):
MIKE GLENN, MHA, Chief Executive Officer; JOSEPH MATTERN III, MD, FAAFP & HMDC, Chief Medical Officer; TINA TONER, RN, MSN, MBA, CENP, Chief Nursing Officer; BRANDIE MANUEL, MBA, CPHQ, Chief Patient Safety and Quality Officer; JENN WHARTON, PT, MHL, Chief Ambulatory and Medical Group Officer; JACOB DAVIDSON, MHA, FACHE, Chief Ancillary and Support Services Officer; TYLER FREEMAN, MSA, CPA, CHFP, Chief Financial Officer. (Not pictured, ALLISON CRISPEN, Chief Human Resources Officer)
Suzanne describes a gradual and insidious decline in staff morale that’s emerged since 2014-2015, most notably when the SLG Chief Ambulatory and Medical Group Officer began restructuring the clinics and family practice offices. Then the hospital stopped hiring part-time nurses.
Using ever sharper pencils, the SLG further streamlined by cross-training, deleting existing part-time positions (firing those who couldn’t work full time), cutting overall positions in each department and not hiring new staff — even when there were qualified applicants, Suzanne reports. Set schedules, the likes of which make life predictable for days off and family time, were eliminated. Plans to attend important rites of passage like graduations, weddings and funerals became a luxury of the past.
Scheduling and the loss of part-time positions created wide-spread disgruntlement throughout the facility. Complaints from staff were met with “you just need to figure out why you want to work here, or you can leave.”
Senior nurses pleaded with management for more staff and part-time positions, citing their own recognition that if their concerns were ignored, there would be an escalation of safety issues that could harm patients and the hospital’s bottom line and reputation.
There was also the phenomenon of what has come to be known as “compassion fatigue” in overworked and under-supported staff. Suzanne says “We’re caregivers. We don’t want to make the hospital look bad.” So the nursing staff shouldered more and more responsibility, working long days without breaks, sacrificing their own welfare for the sake of patient care and hospital optics.
She reports that managers began to look for excuses to ship patients out for care. Surgeons were being pressured to hurry it up. Staff witnessed nurse managers asking, mid-surgery, “how much longer do you think this will take” and providers being told “you’re taking too long to do surgeries.” Adding to the pressure, in recent years the number of surgeons has increased as the number of support staff has been eliminated.
The lack of respect and increasing demands have resulted in “running off 20 nursing assistants” in the last few years, according to Suzanne. They were being asked to care for too many patients. Changes that could be implemented to maintain staff and improve morale — set schedules, retention bonuses, compensation for extra shifts — have not been forthcoming.
“Human resources,” a risible term for working people, is at a crisis point in healthcare. Efforts by institutions to run lean has led to many nurses abandoning the security of steady work in a familiar place close to home in favor of hitting the road and hitting it big with travel nursing.
According to this 2016 article on the trade website TravelNursing.org, nursing shortages began with the 2008 financial crash. The CEO/president of the American Association of Colleges of Nursing (AACN) was quoted back then, saying:
“At AACN, we are most troubled by the shortage of nurses prepared at the baccalaureate and graduate levels since research shows that having enough of these nurses is important to lower patient mortality rates, reducing medication errors and realizing other positive care outcomes.”
At the time, nursing schools were turning away qualified applicants because the schools lacked “faculty, clinical sites, classroom space, preceptors and [had] budget constraints.”
Fast forward six years and the unnatural disaster surrounding Covid, and those highly trained, veteran nurses — the shortage of which so troubled the AACN — now often find themselves working alongside novices with decades less experience who are being paid three to four times as much.
Raises for Me, But Not for Thee
The battle for pay increases at Jefferson Healthcare has been epic, with mediators arguing on behalf of nursing staff for the most niggling little bump. Management maintained that “it’s not sustainable to pay more.” Retention became a major issue, with experienced staff leaving to work elsewhere for single digit increases and the perennial issue of scheduling. During labor negotiations in November 2021, the contract was delayed because the SLG was
“philosophically opposed to raises
for nurses in the top five steps.”
Philosophically opposed. Well, at least they had a philosophy.
There is a seniority tier system in nursing, with the tiers varying from hospital to hospital. Each year of experience is called a “step.” There are 32 steps to reach the apex of the nursing world at Jefferson Healthcare. Random steps are called “ghost steps,” a pause year that precludes pay increases.
After another grueling round of mediated negotiations, the latest contract was finally ratified three weeks ago, on June 22nd, 2022. Despite management’s philosophical opposition, all of the nurses got at least a 4% raise. Ghost step years now pay modest increases instead of none.
Suzanne reports, “The time spent to get there was very disappointing and disheartening. The nurses were made to feel unworthy and expendable.”
In stark contrast, CEO Mike Glenn’s 6% raise three months earlier sailed through the board with only one commissioner, Matt Ready, opposing. [Ready maintains a creative blog of his experience as a Jefferson Healthcare Commissioner.]
Glenn’s pay package is now around $380,000. The rest of the SLG incomes range from a quarter to a third of a million dollars, most of them paid as much or more than Washington’s Governor.
In addition to public record request responses from Jefferson Healthcare, the Free Press has received news tips from stressed nursing staff, current and former, all of them requesting anonymity for obvious reasons. The following are excerpts from a variety of these sources:
“The ACU Staffing Crisis is management created. The Restructure and the stress of Covid-19 are not the root causes of the mass exodus…”
“I understand staffing ICU, especially at night, has been a challenge, however untrained and unqualified staff are being used to staff ICU in unsafe ways that risks liability and patient safety especially when taking into account ICU patient census and telemetry monitoring obligations. It seems the expected standards for ICU care have become adulterated recently with untrained staff for the amount and the acuity of patients we have been having. As I mentioned above, I am all for cross training willing and able nurses to ICU, it just needs to be done correctly with consideration to ICU census, patient acuity, telemetry patients, and number of qualified staff. I’m more than happy to discuss this further and assist in any way. My apologies for the long winded email, I’ve been stewing on this for a couple days now. I can only imagine the amount of similar emails you have been receiving. I’m just rather concerned for the reasons listed above; and my co-nurses, I am sure, share the same sentiments as well.”
— ICU RN, Feb. 2022
“I came onto shift this morning as Charge RN and am receiving no report on the patients. I have never come on and gotten no report in 7 years. Last night one set of patients had 3 nurses covering in succession. When I came on shift Monday the same thing happened and the set of patients I received had 3 different nurses in a 12 hour period. I had to round to the patient and family members who were upset because the care plan was not followed and a comfort care patient inadvertently had oxygen placed on her, which they did not want. I had to explain it was because of the staffing that information did not get across as it should have. This patchwork planning is having impacts on our patients and our staff. It is unsafe. We also have a new nurse for ICU who was put on the floor with no orientation. He spent hours running back and forth to ICU getting supplies because he did not know where they were on ACU [Acute Care Unit]. The standard of nursing care here is actively deteriorating and it makes me uncomfortable.”
— Charge Nurse, Feb. 2022
“The staffing on night shift is unsafe. From the time of the restructure, travelers not fully oriented to our hospital have had to work independently monitoring tele [telemetry] , managing FBC [Family Birth Center] or ACU RNs in the ICU. During many of those times, Telemetry was not documented per policy…
The restructure and the administrations refusal to set templates, or allow self-scheduling, forcing part time employees to take full time positions have left us relying on per diem RNs and travelers. In the ICU, we now only have 3 full time RNs and 1 part time. The rest are employees who have switched to per diem in order to control work-life balance. We are woefully understaffed because of their hubris and arrogance.”
— ICU RN, Feb 2022
“I am not sure if you are aware of this, but the current ACU and ICU staffing situation is very bad. Dayshifts and nightshifts.
It is difficult to see that there is any management involvement in providing real solutions. We just hear about increasing ratios. That will NOT be safe. Over night we had a very busy floor with lots of cognitively impaired impulsive fall risk patients, and only one CNA [Certified Nursing Assistant] available as the other one is stuck as a sitter with our 1:1 resident. The ICU was slammed all night last night and needed assistance that I could not always provide while also assisting the floor. There was an FBC nurse sitter there silencing Teles because the ICU Nurses were so busy.
This feels very dangerous. What is going to happen next week when surgery goes up to full speed and you lose another full-time nurse? We’re drowning here.”
— RN, Feb. 2022
“From 2017 onward, as management initiatives evolved and pressures increased, morale began to decline and the scheduling method changed. As time went on, I watched as we hemorrhaged CNAs (30 in less than a year at one point) and the nurses continuously expressed their discontent and began to leave too…
The lowest hanging fruit to improve morale and to retain staff is to give the nurses a REGULAR SCHEDULE… Please know that the [employment] contracts are attached to PEOPLE. People with lives and families. Well-educated and hard-working people who care about taking care of patients. People who actually WANT to work at Jefferson Healthcare (and would come back) except they just can’t take the mismanagement anymore. They are exhausted by the irregular schedules… and the disregard shown for their work-life balance… nurses that are left are disheartened and do not believe that there is any hope for change. Some of them biding their time prior to retiring, others are actively looking around at other hospitals. I am watching as warm bodies are leaving, first year nurses be pushed into the Charge Nurse Role, being robbed of developing their clinical foundation. Doesn’t this seem dangerous to you?
The ACU Staffing Crisis is management created. The Restructure and the stress of Covid-19 are not the root causes of the mass exodus…
I understand that this is just part of a very complicated issue with this hospital system and there are many pressures from all sides, but it is tough to run and grow and maintain a basic safety level if your staff is gone.”
— RN, Nov. 2021
“I left as I didn’t want the Jab, nor did I want to put a religious exemption in as I fully believe that my right to choose not to have the Jab was exemption enough… employee health is struggling as they don’t have enough staff… I wish more nurses would come forward.”
— former Care Team Specialist, JH Home Health & Hospice, Oct. 2021
Management Response
SLG Chief Nursing Officer Tina Toner offered this response to emails she’d received from nursing staff, including some of the above:
“I want to acknowledge the real challenges we continue to be faced with in terms of staffing. Please know, it is ever apparent that you and everyone of our team is doing all they can to help support their department and care for our patients. I hope that you know that as nursing leaders we are also doing all we can to support staffing, recruitment and retention. When we do have days with less-than-optimal staff our staffing coordinator, the House Supervisor Team and department leaders are all aware. Each morning at 0815 our team comes together to discuss staffing for the next 24 hours so we can collectively work on solutions. This is in addition to time spent looking ahead over the several days and weeks into the future and evaluating the need for additional staff. I know that this is hard, everyone is working hard, and we are all tired. Please, let’s continue to work on solutions, together, I know we will find them. Thank you for all you are doing!”
In the past, nursing and other staff could reach out to board members to share issues and concerns that weren’t being dealt with by their supervisors. Apparently, as the complaints increased, management’s tolerance for that approach trended in the opposite direction. Late last year the board passed a new bylaw that requires all staff complaints and concerns to be copied to the board chair and/or the CEO, thus making the complainant a potential target for retaliation from the very people who aren’t fixing the problems being complained about. No wonder staff dummies up, or leaves to work elsewhere.
A public records request I submitted recently disclosed that Jefferson Healthcare conducted a survey entitled “Employee Engagement 2020,” covering the time period of October 20, 2019 to October 20, 2020. The resulting 46-page document revealed gratitude for co-workers, a modicum of satisfaction and appreciation for the facility, and a substantial amount of frustration and mistrust towards management.
Granted, that was a singularly difficult year for everyone, particularly those in healthcare fields. However, the vast majority of complaints were not Covid-time specific, rather referenced embedded institutional norms of disparity and upper echelon cliques that have resulted in a disabling rift between the worker bees and the bosses.
I’ll share that document with our readers and highlight key aspects in the next installment of this series shortly, along with an overview of the Jefferson Healthcare’s proposed “Campus Modernization & Expansion Project.” On July 20th, the SLG gives one more update to the board before they vote on Wednesday, July 27th, whether or not to take this project to the voters in the form of a bond measure in November.
One can only imagine how beleaguered staff choked on the CEO’s words at the top of this article. A demand for transparency is in order. Should the administration be required to get their house in order before they build another house?
——————————
Updated July 16, 2022
Top photo by Sebastian Eggert
by Stephen Schumacher | Jul 12, 2022 | General
The Port Townsend City Council’s July 5 meeting centered around a potentially wide-reaching project to calm speeds by replacing double-lane streets with single-lane two-way “edge lane roads”, following a revealing Public Works experiment performed on Blaine Street.
The meeting began quietly as council recused itself into executive session for 15 minutes to discuss the legal risks of a proposed action. Upon council’s return, Deputy Mayor Amy Howard as chair opened the meeting up for general public comment.
Stephen Schumacher urged continued attention to police staffing issues. Again seeing only one other unmasked face in the room, he summarized how much-cited CDC mask effectiveness claims are based on cherry-picked data, exposed by a new Lancet review of the full data set showing masks actually increased cases, echoing randomized controlled trials finding masks provide no significant viral infection protection. Lying with statistics undergirds masking propaganda, obfuscating the fact that viruses freely flow through and around conventional face coverings.
City Manager John Mauro responded to public comment by noting that the CDC recommends masking but it is not required, so people can make their own choices.
The first action item was a public hearing on Resolution 22-029 to adopt the 2023-2028 Six-year Transportation Improvement Program (STIP). Public Works Director Steve King explained that each year the city must submit its STIP to the State listing proposed projects and costs so they can be eligible for grants, since needs typically exceed available funding. This year’s STIP identified 47 projects costing $93 million. Councilors Ben Thomas and Aislinn Diamanti moved and seconded, then the resolution passed unanimously.
Idle Ban Again
In unfinished business, Ordinance 3292 banning 3+ minute vehicle idling on property open to the public came back for a second reading, having added emphatic intent language that:
The City Council encourages education rather than penalties in the enforcement of this Chapter, particularly for first offenses.
In public comment, Schumacher said he’s not thrilled about the freedom aspect of criminalizing what people do inside the privacy of their own cars. There are endless good reasons why someone might want to idle for more than 3 minutes to keep warm, recharge batteries, etc., and this measure disproportionately affects elderly and disabled people. It’s unlikely anyone will get charged given the numerous exceptions, but having victimless crime laws on the books is a dangerous practice that can lead to selective enforcement. Perhaps a health case could be made for restricting idling in congested areas like school pickup zones, but not elsewhere. He wished one of the student initiators could have attended council to advocate for their proposal.
Thomas echoed some of this comment, appreciating text added to clarify “the point of this is to educate not to penalize”; he still feels a little torn, but it’s great that kids are getting involved.
Councilor Monica MickHager felt likewise, thanking staff for hearing council discussion by adding a really nice ending sentence under Intent; she shared her surprise finding herself no longer idling while waiting for coffee now that she “got educated.”
Councilor Libby Wennstrom described similar educational benefits seen while waiting at ferries, dumpyards, and banks.
Howard related catching herself doing the same thing; she appreciates this now being in the forefront of her mind and hopes it will land in the forefront of others’ minds as a very small thing that can be done.
MickHager moved, Wennstrom seconded, and the finalized ordinance adding Chapter 10.08 to the PT Municipal Code passed unanimously. Howard drew laughs by quipping, “If the kids were here, they’d give it a round of applause.”
Staffing Resolutions
Several ordinances and resolutions were designed to beef up and reorganize staffing and its compensation:
- Ordinance 3293 replaces the Deputy Clerk (sharing the City Clerk’s meeting and records management duties) with a Public Records Officer (PRO) specializing in responding to increasing Public Records Requests and storing accessible digital records, allowing the City Clerk to focus on meeting management. The timing is good while both Clerk and legal assistant positions are open. Councilor Owen Rowe asked whether Clerk and PRO would be cross-trained, which City Attorney Heidi Greenwood answered affirmatively. Rowe moved to waive council rules to allow approval at first meeting, Thomas seconded while thanking staff for thinking outside the box, and the ordinance passed unanimously.
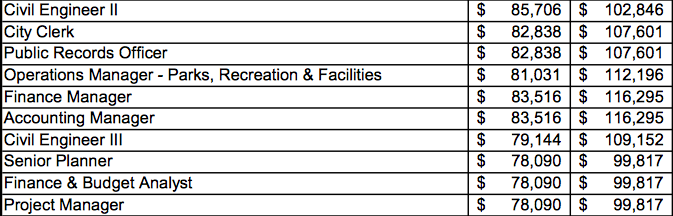
- Resolution 22-030 further reorganizes by replacing the Finance and Budget Analyst (making $78,090-$99,817 per year) with an Accounting Manager ($83,516-$116,295), and the Public Works Project Manager ($78,090-$99,817) with a Civil Engineer II ($85,706-$102,846). MickHager asked the difference between a Civil and City Engineer, so King clarified that a Civil Engineer II is a licensed engineer with a low number of years of experience, Civil Engineer III has more experience, and City Engineer includes managerial competence. Wennstrom noticed the “pretty big” salary range change, so asked about the budget impact if the city hires at the top end for both of these; Finance Director Connie Anderson responded that increased levels of responsibility justified that, and vacancies this year are helping to cover amounts in 2023. MickHager appreciated the great job restructuring and moved to approve. Diamanti seconded, and the resolution passed unanimously.
- Resolution 22-031 authorized a 2022-2023 Teamsters Union contract for police wages and benefits, as negotiated by Anderson, Human Resources Officer Pamela Martinez, and Chief Thomas Olson (all present for this agenda item). Mauro said collective bargaining agreements are complex, so he was glad to have this team on it. Anderson said the emphasis was on retention and recruitment. Wennstrom noted wages changes start July 1, while benefits became effective January 1. MickHager moved, Thomas seconded, and the resolution passed unanimously.
- Resolution 22-032 authorizes an accounting contract up to $35,000 with CPA firm TDJCPA. Anderson noted the city was missing a Finance Manager since last summer until a replacement was hired in January and Anderson arrived in March, so TDJCPA would help her fill that gap, put in controls, and build her team going forward. Wennstrom asked if this was included in the budget and would be ongoing. Anderson answered it was not in the budget, but the money is already covered by a position not yet filled; whether to renew will be re-evaluated, since TDJCPA provides a lot of services to fill in gaps for small communities. Rowe moved, MickHager seconded, and the resolution passed unanimously.
- Long-line road stripe repainting was contracted out to the low bidder despite being $25,000 over budget due to pent-up demand and significantly higher fuel and paint prices. Wennstrom moved to proceed with reduced project scope per staff recommendation, Thomas seconded, and council approved unanimously.
ADU Parking Relief Delayed
New Planning Director Emma Bolin turned it over to Planning Manager Judy Surber to report back about amendents to PT Municipal Code 17.72 requested by council on March 14 to eliminate ADU parking requirements. The Planning Commission asked to broaden the scope of parking-related changes to include boarding houses, multifamily homes, B&Bs, etc.
Rowe and Diamanti were concerned how slight a delay this would be for their ADU priority, and agreed that anything arising that might bog down the process should be skipped. Thomas wanted a time limit, and Diamanti suggested 3 months.
Wennstrom wondered whether parking places should always be required to be paved with gravel and asphalt; the goal was to make it easier for existing dwellings to add an ADU, but current parking requirements make that harder.
MickHager proposed just keeping it focused on ADUs and doing that well. Diamanti responded that she understands staff’s preference is to combine changes as a more effective use of resources, which Surber confirmed. Howard was disinclined to stop the Planning Commision from doing this work.
Wennstrom moved to task the Planning Commission to explore other parking code amendments in tandem with ADUs with a request to get back to council by November 2022. MickHager seconded and the council concurred unanimously.
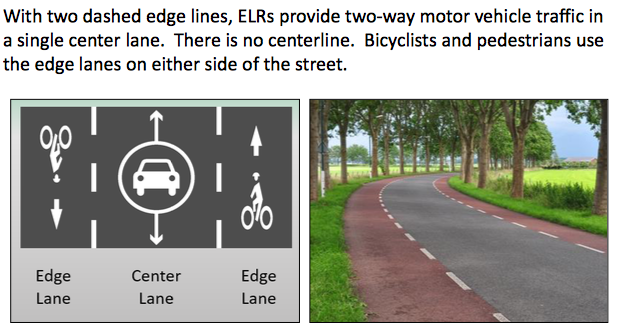
Edge Lane Roads Presentation
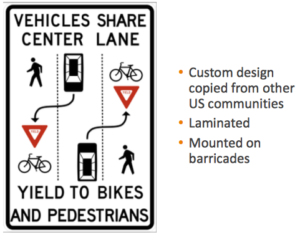
Public Works Director King and his staff explained Edge Lane Roads (ELRs) as a tool to address public concerns about street repair conditions and traffic calming.
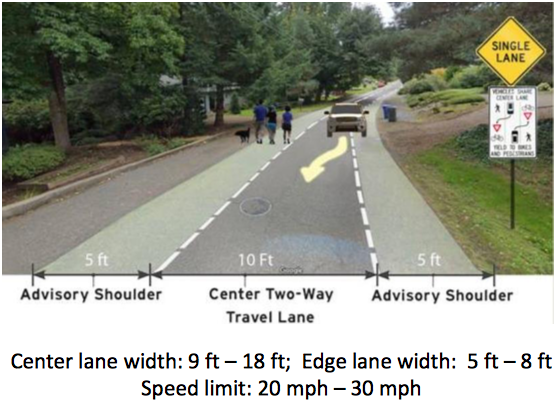
ELRs turn narrow roads where folks often walk into explicitly single lane roads, forcing cars to slow and negotiate any obstacles like oncoming traffic, pedestrians, bicycles, and deer. They work better as two-way roads to make folks more cognizant of slowing down for safer passing. Installation costs are less than adding pedestrian/bicycle shoulders or concrete sidewalks.
Most important for preservation of our pavement, with streets decaying from the outside in, ELRs give the remaining pavement a longer life, as vehicles no longer drive on the edge of streets.
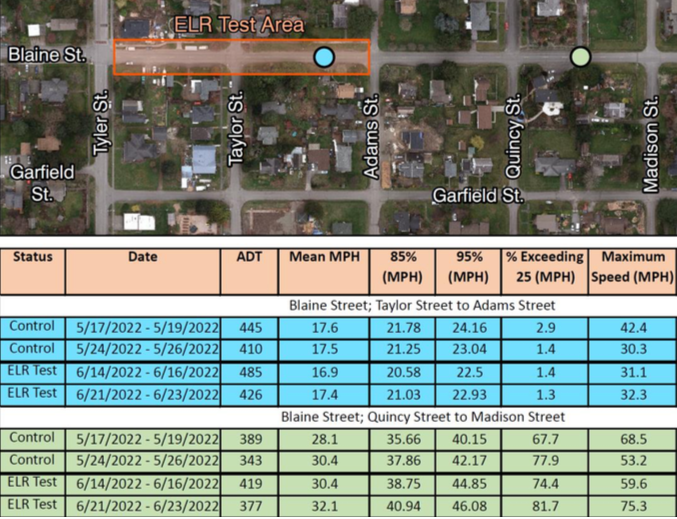
Edge Lane Road Experiment on Blaine Street
Public Works installed an experimental Edge Lane Road on two blocks of Blaine Street between Tyler and Adams at the cost of $1,000 plus $15,000 for initial engineering, outreach, and research.
One thing Public Works would have done differently would be to put the doorhangers up before the temporary lane was put on Blaine. But there were good discussions afterwards and better understanding after explaining this is now just a single-lane road.
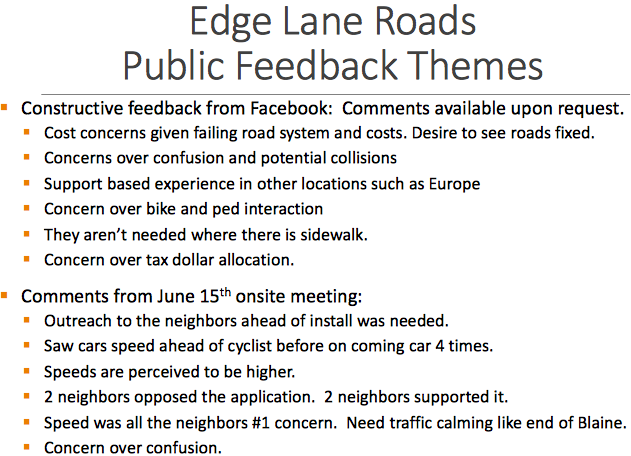
Neighbors shared a variety of comments and observations, such as:
- Why do this for an area that already has a sidewalk (not much used because it ends)?
- One of the neighbors saw 4 times that a car sped up to get ahead of a pedestrian.
- Another neighbor said speeds are now higher (perhaps not borne by data readings).
Speed monitoring revealed some curious and troubling results: average speeds dropped slightly inside the ELR Test Area, but grew substantially a block away, maxing out at 75.3 MPH!
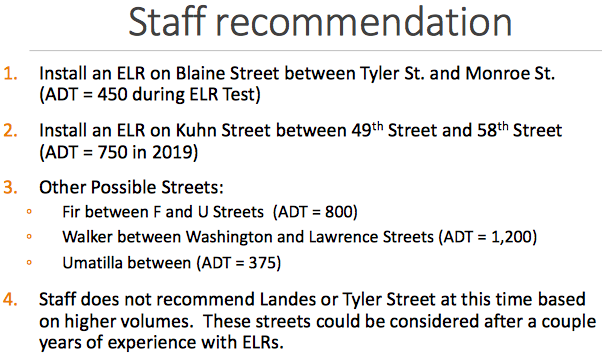
King recommended keeping ELRs on streets with volume lower than 2,000 trips a day, at least to start, focusing on high pedestrian streets needing shoulder restoration. Due to the relationship between speed and severity of accidents, there’s big drop-off of dangers at 20 MPH compared to 25 MPH. Edge Lane Roads are a new tool, and staff appreciates feedback.
Edge Lane Roads – Public Comments
In public comments, Dan Burden said he went out three times to record what people were doing and what they thought, which was all positive. But what people saw was no change in speed, which surprised him. What’s wanted with traffic calming is to bring down the higher range of speeds. Burden offered great compliments to staff, since less that 1% of cities are doing this.
Schumacher thanked staff for opening his mind to these new ideas, but he’s concerned about arterials being deprecated. He related his experience attending a traffic planning meeting in the 90s where experts advised raising the speed limit on arterials like 19th Street to match the natural speed most people were driving, but the police chief vetoed the idea. There should be a balance to keep things moving along the arterials while making the backwaters safer. He’s also baffled by the 85% percentile speeds on Blaine from Quincy to Madison going up from 37 MPH (!) to 40 MPH (!!) right outside the ELR test region, since he hardly ever sees people drive more than 5 MPH above the speed limit in town.
Scott Walker said he’s generally supportive of the idea. In Austrialia, outback highways are one lane with shoulders, so if you see a truck coming, you move to the side, which works better than two lanes. He emphasized that paint is not a substitute for a physical separator. Blaine is a highly used street to get to Chetzemoka, so folks shouldn’t be asked to walk in the streets. Howard Street from Hastings to 35th has a huge amount of bicycles and pedestrians.
Edge Lane Roads – Council Comments
Thomas wondered what areas in town have more than 2,000 car trips per day; King replied that Landes Street by Safeway gets that. Thomas also wondered if striping would lead to more parking in ELRs.
Diamanti and Wennstrom asked about the $15,000 engineering cost; King replied that was the budgeted internal cost as if it came from an external engineering department.
Wennstrom asked about the 75 MPH maximum speed detected during the test. King replied it was an outlier, but staff was shocked and checked the equipment was working correctly.
Councilors brainstormed other parts of town they’d like to install ELRs, springing off of staff’s recommended list.
MickHager was glad Landes was taken out, but would like ELRs added in the areas around Castle Hill, Howard Street, McPherson Street, and Hancock Street near Memory Lane.
Wennstrom suggested one on Sheridan Street between Hastings and Umatilla. Rowe suggested around Cherry and Redwood Streets; he supports continuing with this and hopes it does become something accepted in town.
Thomas asked whether these are as good as a two-lane road with bike lanes on each side for safe bicycle usage. King replied that depends on the specific situation and condition of the shoulders; for streets like F Street it’s important to have separated bike lanes per Walker’s comment.
MickHager said she’s for this idea, and was very surprised that she didn’t get one positive response from anybody in her community! She wonders how to spread ELRs diversely to the community out into places like Castle Hill and North Beach, because most of the sites on the list are in the older part of town. She thinks people could get used to them if they were put in popular roads like 14th Street.
MickHager continued jokingly that she’s glad “you’re going to lower the speed limit to 20 miles an hour; please could we do that on all our streets? That’s how I feel about it. My family does not talk to me anymore, because that’s how I feel about it. They think I’m crazy, but I’m not!”
Wennstrom said that having cars parked on the side of streets in residential neighborhoods helps with traffic calming. She noted that 80% bicyclists on San Juan Avenue ride on the sidewalks rather than on the bike lanes. She laughed in incredulity that, “Wow, we took out all this parking and built these big huge bike lanes, and right on the sidewalk!”
Diamanti said that feedback has been a lot more favorable than the infrastructure committee was afraid of when they first started talking about ELRs. She thinks it’s a really smart option and a chance to be leaders.
Howard joshed that “she sincerely hopes whoever was driving 75 was experiencing some sort of an emergency, and not having a temper tantrum because we forced them to do something new.” She did try driving it herself, and the hardest part was the signage, which was too small if you were driving, so you had to slow down to look at it.
Howard added that the biggest problem is Americans are fiercely individualistic and try to get their car in front of others’, so we need to make this a community culture thing where we share our streets and make them accessible to everyone, which should be part of the messaging. She would like it if ELRs discourage giant delivery trucks: “Maybe narrowing it they’ll have a harder time and won’t use that one as much, preserving that pavement quite a bit.”
Wennstrom concluded that “it’s an educational opportunity. I remember, when we were first talking about putting in roundabouts, the screaming and yelling… and now people have pretty much got the feel for the roundabouts and see the value. So getting past that initial ‘whoa, that’s scary and weird,’ and some familiarity before it happens in your neighborhood, I think is a great idea.”
Closing Reports
Deputy Mayor Howard announced her election to the Board of Directors of the Association of Washington Cities.
City Manager Mauro reported about recruiting clerk, public records, and police officers. The city’s 2023 Workplan Retreat is being held Monday, July 18, 10am-4pm at the Northwest Maritime Center, and any member of the public is free to attend. The city is part of an electric network consortium getting a $4 million grant to build up fast chargers for electric vehicles.
Mauro ran through updates on large capital projects including Discovery Road, Kearney Street, Lawrence Street, Chetzemoka kitchen shelter, library, golf course, and optimizing City Hall for comfort and efficiency.
by Jim Scarantino | Jul 9, 2022 | General
Suicide and substance abuse touch all our lives. These horrors and tragedies surround us.
In my eight years in this town, I have personally known one young man who hanged himself, and I’m friends with people whose relatives have taken their lives in what should have been their prime years.
I found one suicide victim, a man who had veered off the road intentionally to collide with a tree. I won’t forget opening that crumpled door, feeling for the pulse that wasn’t there and saying a prayer as I awaited the emergency services response. First responders and loved ones and friends found the other suicides and those who died by overdose.
I helped with the funeral service for the young man who hung himself outside Manresa Castle. He had a severe opiate addiction. He was living at the Mill Road transient camp, as it was then known (now called the Caswell-Brown camp after two people found dead in our community.) About 200 mostly young people attended that service.
The young man’s drug dealer was stopped at the door to the church because he attempted to smuggle in a small dog under his shirt. He was there to score, not mourn. Having just been released from jail, he didn’t have any of his own dope. According to a substance abuse expert who was in attendance, about half of the 200 people were addicts. Some had come drunk, and I found an empty vodka fifth in a waste can. Others were high. As I was closing up that evening I noticed two cars parked at the very edge of the church property. I almost tapped on a window but stopped when I saw people inside shooting up.
A funeral for an addict who had died by his own hand or overdose was sadly nothing new. I wonder how many of those troubled souls have since overdosed and/or contemplated or attempted suicide.
Our community’s hidden suffering, hopelessness and despair is expressed in these deaths. Yet the question of whether Lombardy poplars should be felled draws more attention and passion than these tragedies. Trees along Sims Way have been given names; the suicides and overdose fatalities are nameless to the general public.
Maybe in rarefied circles in this community some can claim they have no personal connection with anyone or any family that has lost someone to despair and drugs. I don’t believe them, any more than the city council member who told me he has no one in his family or circle of friends suffering from addiction.
A death like that of Jarrod Bramson, the popular musician whose death was attributed to homicide by his drug dealer, is not far removed from the category of suicide or fatal overdose. It was a fatal overdose, just not administered by Jarrod himself. Maybe it can be considered assisted suicide. Isn’t that descending spiral of addiction and substance abuse little more than a slow suicide? Are not every one of of the dealers handing out Fentanyl pills assisting suicide?
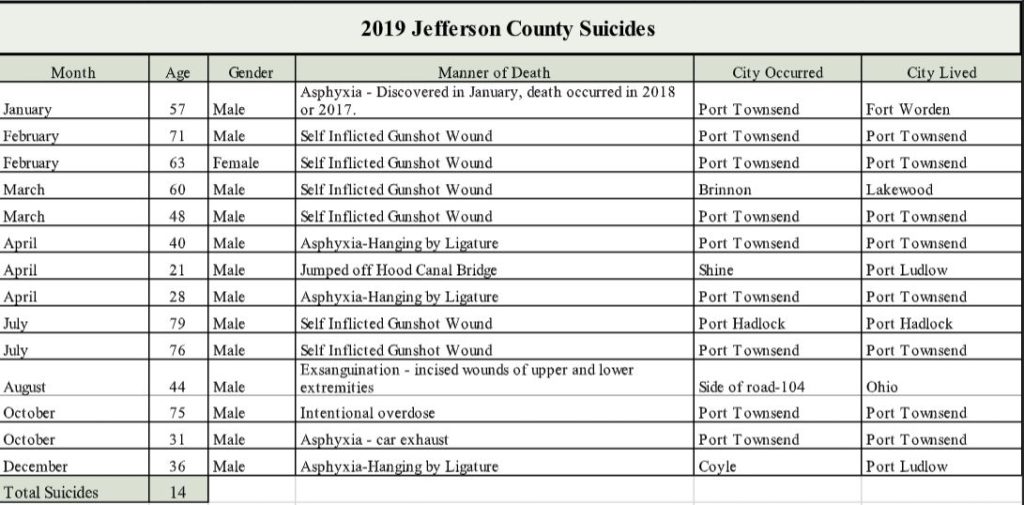
County Prosecutor James Kennedy’s office has provided at my request what is a colorless inventory of suicides and fatal overdoses in Jefferson County. The identities of the deceased are shielded according to state law. Those tables are found below.
Suicides in Jefferson County 2003 to Present
(click here for full table)
Partial screen shot of information complied by Jefferson County Prosecuting Attorney Office at Port Townsend Free Press request.
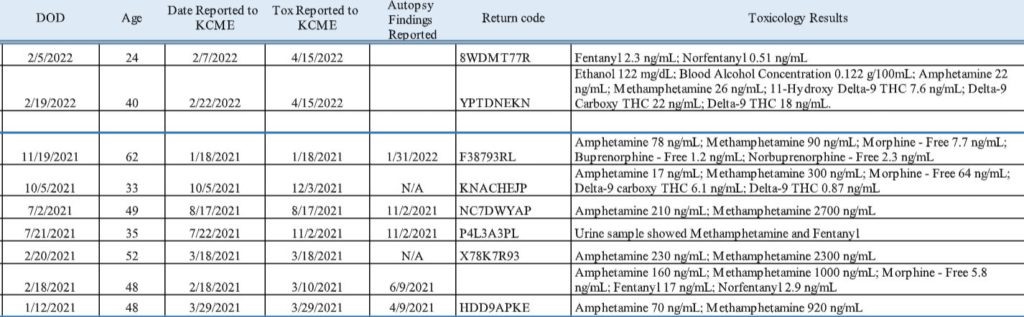
Fatal Overdoses, Jefferson County, 2019 to Present
(click here for full table)
Partial screen shot of information complied by Jefferson County Prosecuting Attorney Office at Port Townsend Free Press request.
Prosecutor Kennedy writes,
“[T]he true picture is murkier than the numbers. For example, it is not uncommon to come across a person who has committed suicide, by gun shot or hanging, for example, where drug (and/or alcohol) paraphernalia is present. We usually test the decedent’s blood for drugs in those cases and the results are almost always positive. We typically classify these deaths as a suicide even though drugs clearly played a significant role in the death.”
Kennedy continues,
“Other times we have come across long term drug users who die after having ingested a significantly higher amount of drugs than they typically use. What they ‘typically’ use is often hard to pin down with certainty — if available it comes anecdotally from acquaintances — but the inference remains that this was a suicide by drug overdose. However, since we cannot be certain, we usually classify these deaths as we would an overdose, unless there is other indicia present like a suicide note.”
Victoria Brown, age 23, is in these tables. She died of an overdose in the lawless transient camp the County Commission permitted to fester for more than a year at the Fairgrounds. The transient camp on Mill Road that the county has established with OlyCAP is named after her, as well as John Caswell. He died during the heat wave in 2021. I am friends with the man who had tried to help him that day and later found him dead by a picnic table off Sims Way.
Caswell’s death cannot be detached from his substance abuse. He had been drinking alcohol in the oppressive heat, and help had been sought at the hospital to cool him down. The hospital put him back on the street. He was scheduled to enter alcohol treatment in a couple of days. In the meantime, he had to stay “balanced” (as chronic drinkers call it) to fight off shakes, withdrawal and DTs. Is his death a fatal overdose and/or a suicide?
How many other deaths need to be added to these tables? How many suicides have been attempted, how many overdoses have been reversed just short of death? (About thirty 10th and 12th graders report attempting suicide in the past year, according to the 2021 Healthy Youth Survey, on which Port Townsend Free Press reported.)
Prosecutor Kennedy has suggested running down further information from law enforcement and emergency services, saying “this is a really important issue. Thank you for paying attention to it.” I will be seeking to obtain further information on our county’s attempted suicides and non-fatal overdoses for a future report.
by Jim Scarantino | Jul 2, 2022 | General
Twenty-five percent of Jefferson County high schoolers made a plan to kill themselves in the last year. About 30 tenth and twelfth graders tried to kill themselves.
These and other alarming reports of severe mental health problems among the county’s high schoolers were released as part of the 2021 Healthy Youth Survey conducted by the Washington Department of Health. 354 Jefferson County students participated in the study, which also covers all counties statewide.
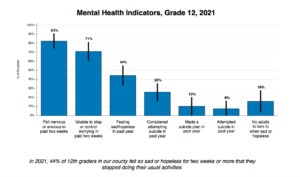
Our county’s youth report crushing hopelessness. 36% of tenth graders reported feeling so sad or hopeless that they stopped doing their usual activities. That pall of debilitating malaise rose to 44% among 12th graders. The DOH’s statewide results show that youth sensing no or only slight hope are twice as likely to consider suicide as youth with a moderate to high sense of hope.
83% of 12th graders reported feeling nervous or anxious in the two weeks preceding the survey, and 71% of them were unable to stop worrying in that time period. The numbers for 10th graders are only insignificantly better.
Among 12th graders, 26% reported (24 students) considering suicide during the year, 10% (9 students) reported making a suicide plan, 8% (7-8 students) reported attempting suicide. Among 10th graders, 21% (30 students) reported considering suicide, 25% (36 students) made a suicide plan, and 13% (19 students) reported attempting suicide.
Statewide, according to DOH, substance abuse reporting is down over 2018, but mental health problems are more widespread and severe. The 2021 survey found that statewide 74% of 10th graders reported feeling nervous, anxious, on edge, or not being able to stop or control worrying, 20% reported they seriously considered attempting suicide, 16% reported they made a suicide plan, and 8% reported they attempted suicide in the past 12 months. The rates for planning and attempting suicide by 10th graders are higher in Jefferson County. Jefferson County 12th graders reported considering suicide and attempting suicide also at rates higher than the comparable state rates.
Readers are encouraged to read the Fact Sheets from the survey for Jefferson County high schoolers. Much more data, some broken down by demographics, is available. You may use this link: Healthy Youth Survey 2021. Click on the Fact Sheets link at the top of the page, then select “county” and pull down Jefferson County. From there you can access many fact sheets on mental health, substance abuse and other indicia of teen health. The 134 pages of survey results cover 6th, 8th, 10th and 12th graders.
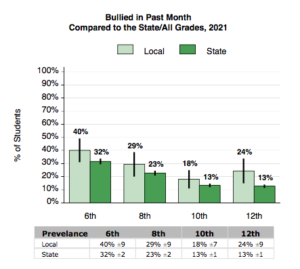
Dozens of graphs in the Healthy Youth Survey 2021 show detailed analyses of mental health indicators, substance abuse and other well-being factors in our community. This breakdown shows a higher incidence of bullying experienced in Jefferson County as compared to Washington State, at every grade level.
Suicide is the second leading cause of death for Washington teens 15-19 years old, the survey explained, and most youth suicides occur at home. Suicide attempts among children even as young as 9 years old is on the rise. As reported by Hannah Furfaro, a Seattle Times mental health reporter:
“A pair of new national research studies and Washington data help confirm what Marshall and many others are seeing in hospitals across the Pacific Northwest. Use of medications or other poisons to attempt suicide or self-harm are rising among youths as young as 9, and the largest increases are among those ages 10-12. The number of kids in that age group who ingested some type of poisonous medication or other substance to attempt suicide increased by 4.5 times from 2000 to 2020, according to one of the national studies, published in JAMA Pediatrics in March, compared to a 2.4-fold increase among older adolescents.”
The 2021 survey found a slight decrease in drug use that may only be temporary. According to Dr. Maayan Simckes, an epidemiologist with the Washington Department of Health, drug use could well increase as teens go back to more normal lives, which involves being able to gather with peers, and potentially partying.
Jefferson County’s Board of Health Response and Action
The 2021 data is nothing new. At its April 2019 meeting, Dr. Tom Locke, then the public health officer, told the Jefferson County Board of Health that the 2018 Healthy Youth Survey results “showed concerning findings in the youth mental health category.” At the following month’s meeting, team members from the Substance Abuse Prevention Program at the Health Department were supposed to provide “a more in depth look at the data from the Healthy Youth Survey.” (Reporting on substance abuse among high schoolers was also cause for concern.)
The Board of Health never returned to the mental health crisis among Jefferson County high schoolers. Instead of considering data that was supposed to be provided by the Substance Abuse Prevention Program, the Board spent its meeting time discussing nuclear disarmament. In the past three-plus years since the county’s public health officer informed the Board of Health of “concerning findings” about youth mental health, the subject has never been an agenda item. The 2021 Healthy Youth Survey results were released in March of this year but have not been discussed by the Board of Health.
The members of the Board of Health are County Commissioners Greg Brotherton, Heidi Eisenhour and Kate Dean; Libby Wennstrom, Port Townsend City Council Member; Kees Kolff, Public Hospital District Commissioner; Sheila Westerman, Citizen-at-Large; and Denis Stearns, Citizen-at-Large.